

Health service use, health outcomes and treatment costs of adults with a cochlear implant: a retrospective cohort study
- PMID: 40340712
- PMCID: PMC12060529
- DOI: 10.1186/s12889-025-22898-8
Health service use, health outcomes and treatment costs of adults with a cochlear implant: a retrospective cohort study
Abstract
Background: Data about the ongoing health service use, health outcomes and healthcare treatment costs of adult cochlear implant users are limited. This study examined health service use, health outcomes and treatment costs of adults who had a cochlear implant.
Methods: This was a retrospective cohort study of adults aged ≥ 18 years who received a cochlear implant during 2011-2021. Linked hospitalisation, non-admitted patient (NAP) services and mortality data in New South Wales (NSW), Australia were used. Health service use, health outcomes and treatment costs were compared for younger (18-64 years) and older (≥ 65 years) adults. A negative binomial regression model was used to examine factors associated with hospitalisation and health outcomes.
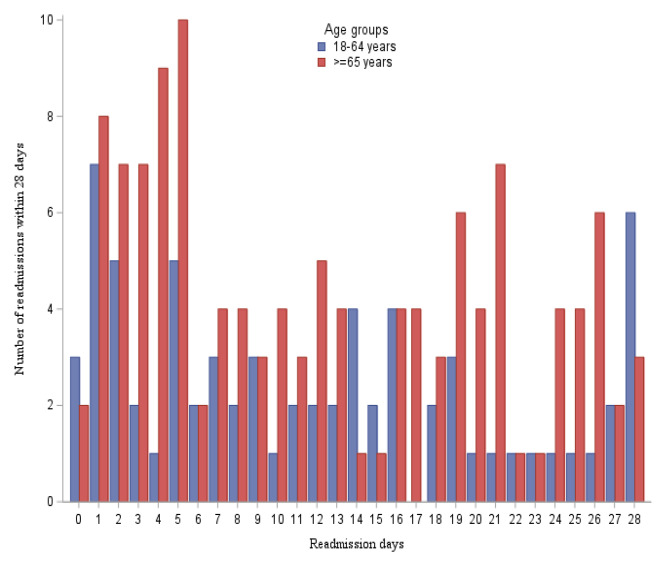
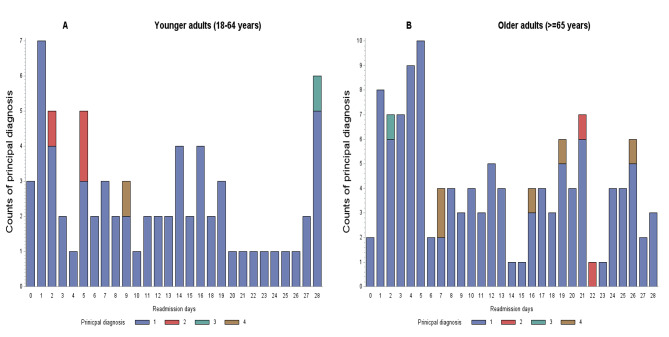
Results: There were 3071 adults who had a cochlear implant; 47.6% aged 18-64 years and 52.4% aged ≥ 65 years. Older adults had a higher proportion of all-cause hospital admissions (34.1% vs. 18.4%, respectively), readmission within 28 days (7.8% vs. 4.7%, respectively), ≥ 13 NAP service contacts (33.9% vs. 24.9%, respectively) and mean treatment costs (AUD$44,101 vs. AUD$41,663, respectively) than younger adults. Charlson comorbidities and mental health disorders were key predictors of both hospitalisations and NAP service contacts for younger adults. Postoperative mechanical complications and prior hospital admissions were predictors of hospitalisation and NAP service contacts, respectively for younger adults. Having ≥13 NAP service contacts and a cochlear implant removed were predictors of hospitalisation and NAP service contacts, respectively for older adults. Having a longer hospital length of stay (LOS) was associated with cochlear implant removal, treatment cost, and other health conditions for both younger and older adults.
Conclusions: Adults with multimorbidity used more hospital-based services or incurred large treatment costs. Early detection and treatment of comorbidities and long-term post-cochlear implant follow-up to identify any potential complications may reduce unplanned hospitalisations, adverse health outcomes, and associated hospital utilisation costs.
Keywords: Adults; Cochlear implant; Health outcomes; Health service use; Treatment cost.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval and a waiver of consent was obtained from the NSW Population Health Services Research Ethics Committee (Reference: 2022/ETH00382/2022.07). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- WHO. World report on hearing. Geneva, Licence: CC BY-NC-SA 3.0 IGO. 2021.
-
- Deloitte Access Economics. The social and economic cost of hearing loss in Australia. 2017. Accessed at: https://apo.org.au/node/102776. Accessed 10 February 2023.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
