

Improving lower-extremity artery depiction and diagnostic confidence using dual-energy technique and popliteal artery monitoring in dual-low dose CT angiography
- PMID: 40341131
- PMCID: PMC12062275
- DOI: 10.1038/s41598-025-97868-6
Improving lower-extremity artery depiction and diagnostic confidence using dual-energy technique and popliteal artery monitoring in dual-low dose CT angiography
Abstract
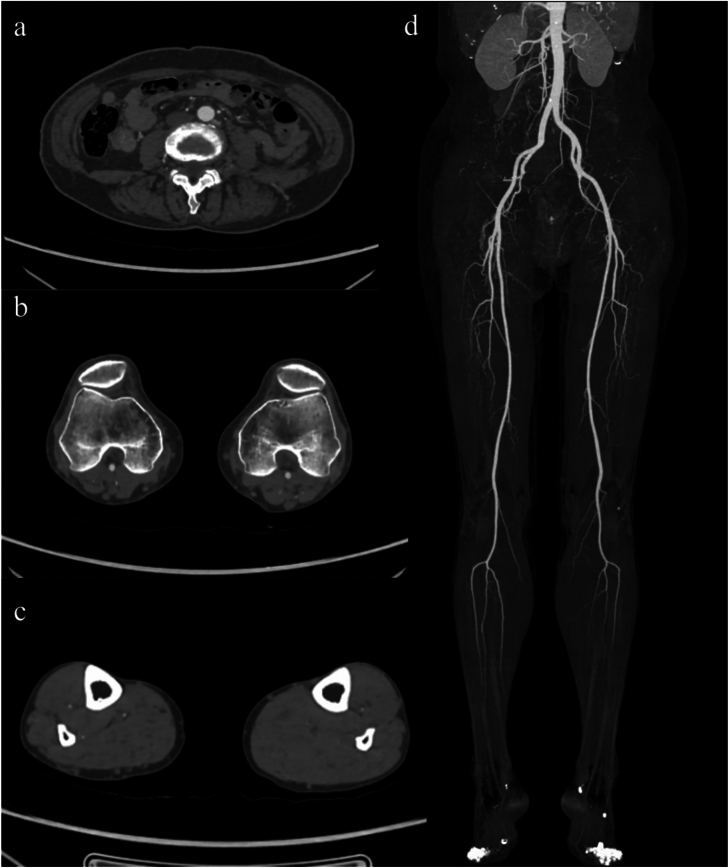
To assess the utility of dual-energy CT scanning (DECTs) with popliteal artery (PA) monitoring in dual low-dose (radiation and contrast) lower-extremity CT angiography (LE-CTA). 135 patients undergoing LE-CTA were prospectively included and divided into three groups of 45 each. Group-A: conventional scanning, 105 mL of contrast, abdominal aorta monitoring; Group-B: low-dose DECTs, 95 mL of contrast, AA monitoring; Group-C: low-dose DECTs, 85 mL of contrast, PA monitoring. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR), as well as their elevations at seven arteries, were evaluated. Two radiologists conducted subjective assessments of overall image quality and vascular diagnosis in three arterial segments. They also recorded the visible branch grading in the lower-knee segment (LKS). Group-C reduced contrast and effective doses by 19.04% and 12.62%, respectively, compared to Group-A (P < 0.001). Group-C had the best SNR and CNR for four LKS arteries. Regarding SNR and CNR elevations, Group-C outperformed Group-B in distal arteries beyond the PA. In the LKS, Group-C performed best for subjective overall image quality, visible branch grading, and diagnostic confidence, as well as the inter-observer diagnostic consistency, followed by Group-B and Group-A (P < 0.001). DECTs with PA monitoring provides excellent depiction of lower-extremity arteries under dual low-dose conditions.
Keywords: Computed tomography angiography; Dual energy CT; Iodine contrast; Lower extremity arteries; Radiation dose.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures





Similar articles
-
Application and significance of precise computed tomography angiography (CTA) scanning technology in the assessment of lower extremity arterial diseases.Clin Radiol. 2025 Jul;86:106933. doi: 10.1016/j.crad.2025.106933. Epub 2025 Apr 17. Clin Radiol. 2025. PMID: 40403343 Clinical Trial.
-
Radiation dose and image quality with new protocol in lower extremity computed tomography angiography.Radiol Med. 2019 Mar;124(3):184-190. doi: 10.1007/s11547-018-0963-7. Epub 2018 Nov 27. Radiol Med. 2019. PMID: 30478814 Clinical Trial.
-
CT imaging using variable helical pitch scanning for lower extremity arterial disease: Reduced contrast medium dose, improved image quality and diagnostic accuracy.Eur J Radiol. 2024 Dec;181:111792. doi: 10.1016/j.ejrad.2024.111792. Epub 2024 Oct 25. Eur J Radiol. 2024. PMID: 39476770 Clinical Trial.
-
Advantages and disadvantages of single-source dual-energy whole-body CT angiography with 50% reduced iodine dose at 40 keV reconstruction.Br J Radiol. 2021 May 1;94(1121):20201276. doi: 10.1259/bjr.20201276. Epub 2021 Feb 22. Br J Radiol. 2021. PMID: 33617294 Free PMC article. Clinical Trial.
-
Improving diagnostic accuracy for arteries of lower extremities with dual-energy spectral CT imaging.Eur J Radiol. 2020 Jul;128:109061. doi: 10.1016/j.ejrad.2020.109061. Epub 2020 May 12. Eur J Radiol. 2020. PMID: 32442836
References
-
- Firnhaber, J. M. & Powell, C. S. Lower extremity peripheral artery disease: Diagnosis and treatment. Am. Fam. Physician99, 362–369 (2019). - PubMed
-
- Hiatt, W. R. et al. Atherosclerotic peripheral vascular disease symposium II: Nomenclature for vascular diseases. Circulation118, 2826–2829 (2008). - PubMed
-
- Fowkes, F. G. et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet382, 1329–1340 (2013). - PubMed
-
- Shwaiki, O. et al. Lower extremity CT angiography in peripheral arterial disease: From the established approach to evolving technical developments. Int. J. Cardiovasc. Imaging37, 3101–3114 (2021). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
