

Treatment outcomes of a Swiss non-infectious paediatric uveitis cohort: retrospective study over ten years
- PMID: 40341441
- PMCID: PMC12062484
- DOI: 10.1186/s12348-025-00458-w
Treatment outcomes of a Swiss non-infectious paediatric uveitis cohort: retrospective study over ten years
Abstract
Introduction: Paediatric uveitis treatment recommendations suggest a step-up treatment approach starting with topical treatment, followed by antimetabolites and thereafter biologics. With this study, we are investigating the safety and efficacy of the current treatment approach in a large cohort.
Material and methods: Single center retrospective study. Patients with non-infectious uveitis under the age of 18 years at first presentation, between January 2012 and June 2022, were eligible for inclusion. Data extracted from the electronic health records included age at first presentation, sex, involved eye segment, visual acuity (VA), complications, associated systemic disease, treatments, and number of consultations. Cases were grouped according to their final treatment regime (topical only, methotrexate, TNF alpha inhibitor, other). VA outcome, treatment response, adverse events, and frequency of consultations were evaluated. The study was approved by the local ethics committee.
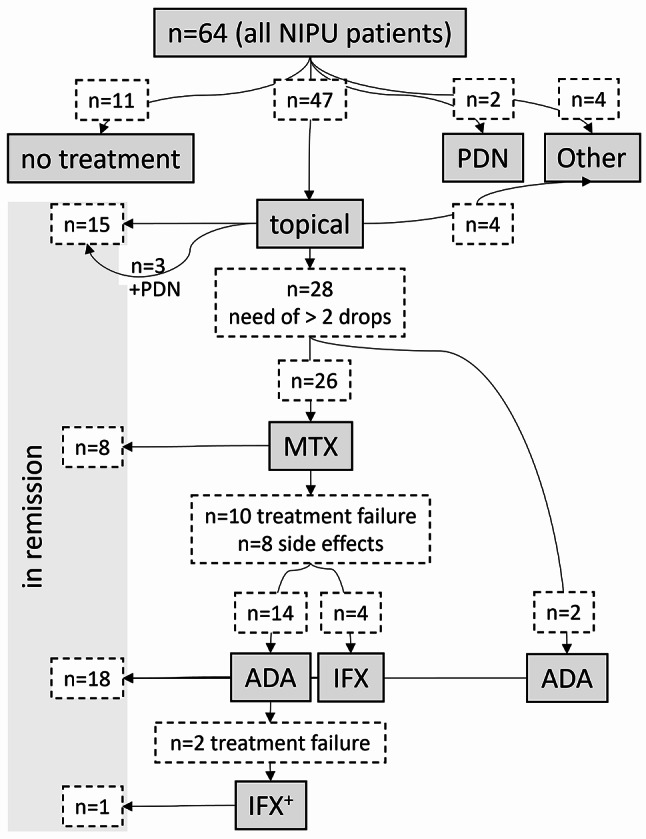
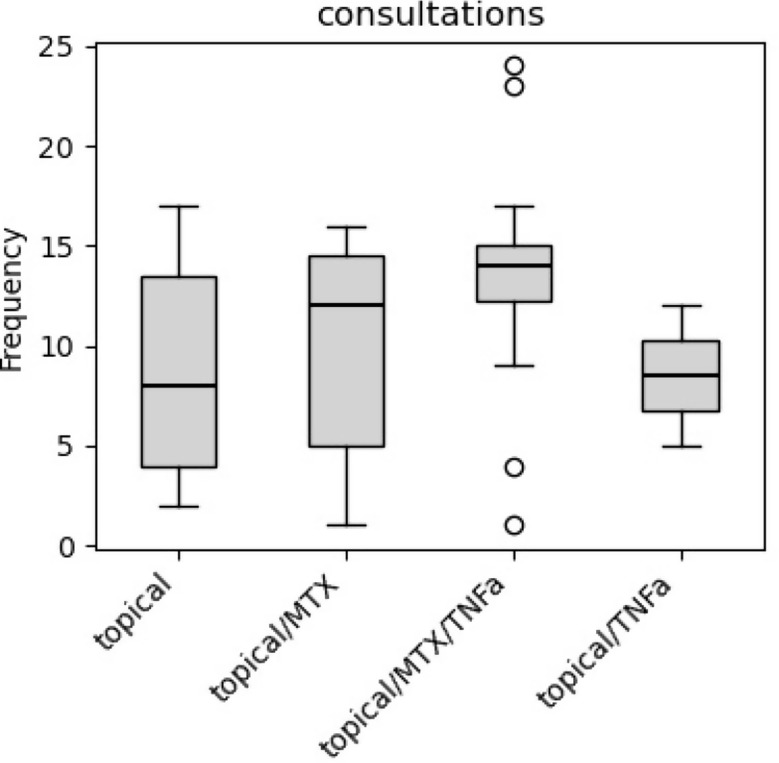
Results: 64 non-infectious paediatric uveitis cases were included. Age at first diagnosis ranged from 2 to 17 years, with a two-peak distribution, 52% were male. Anterior uveitis was the most common presentation, followed by intermediate uveitis, posterior uveitis, and panuveitis. Topical treatment achieved remission in 23%, anti-metabolites in 12%, and escalation to TNF alpha inhibitors in 30%. Alternative treatments or observation only were documented in 16% and 17%, respectively. Median duration from first presentation to the start of anti-metabolite or TNF alpha inhibitor were 115 days and 269 days, respectively. There was a median of eight consultations during the first year of follow up. Frequency of consultations during the first year increased with every treatment escalation. VA outcome did not differ between the different treatment groups.
Conclusion: The step-up treatment approach shows a safe profile in regards to VA outcome. Methotrexate presents a high rate of treatment failure and adverse effects. Adalimumab and infliximab are effective and safe. Timely treatment escalation might lower treatment burden for affected children, their families, and health care providers.
Keywords: Adalimumab; Children; Methotrexate; Paediatric; TNF alpha inhibitor; Uveitis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Local ethics committee approved this study (Institutional review board of Swiss Ethics/BASEC No. 2023 − 00439). The Tenets of the Declaration of Helsinki were followed. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
LinkOut - more resources
Full Text Sources
