

Second-line pharmacological treatment strategies for trigeminal neuralgia: A retrospective comparison of lacosamide, gabapentin and baclofen
- PMID: 40341553
- PMCID: PMC12266635
- DOI: 10.1111/head.14952
Second-line pharmacological treatment strategies for trigeminal neuralgia: A retrospective comparison of lacosamide, gabapentin and baclofen
Abstract
Background and objectives: Carbamazepine is commonly used as the first-line treatment for trigeminal neuralgia, but therapeutic failure due to adverse effects is frequent. While various second-line alternatives have been suggested, there is limited evidence directly comparing these options. This study aimed to evaluate and compare the effectiveness and tolerability of lacosamide, gabapentin, and baclofen in patients with refractory trigeminal neuralgia.
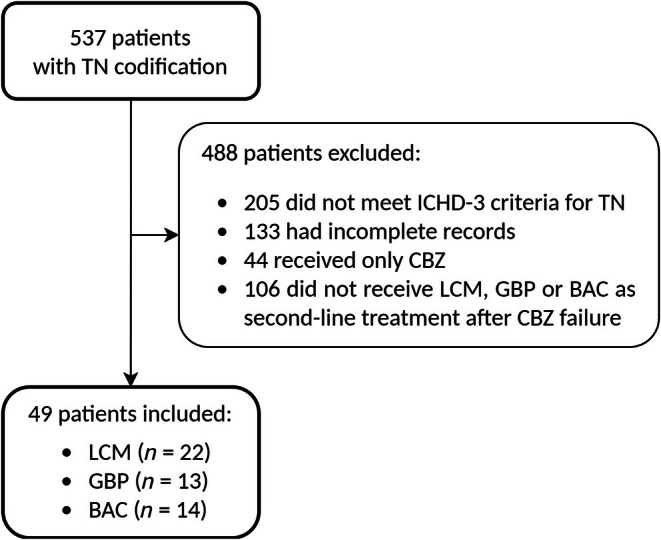
Methods: This retrospective cohort study analyzed patients with trigeminal neuralgia who, after not responding to carbamazepine, were treated with either lacosamide, gabapentin, or baclofen between January 2015 and December 2023. We collected clinical and demographic data and assessed response variables after 3 months of treatment. We compared pain relief (defined as patient-reported pain reduction and absence of additional treatments or emergency consultations within 3 months) and side effects. Secondary endpoints included absence of pain, treatment retention rates, and the need for subsequent surgery.
Results: A total of 49 patients were included, with 22 receiving lacosamide, 13 receiving gabapentin, and 14 receiving baclofen. The mean (standard deviation) age was 62.1 (14.1) years, with 53% female, and the median duration since diagnosis was 3.4 years. Carbamazepine failure was attributed to inefficacy in 76% of patients and intolerance in 24%. There were no significant demographic or clinical differences among the treatment groups, except for the concurrent use of carbamazepine: 68% in the lacosamide group, 54% in the gabapentin group, and 100% in the baclofen group (p = 0.019). Pain relief rates were 68% for lacosamide, 54% for gabapentin, and 64% for baclofen (p = 0.694). Adverse effects were reported in 46% of lacosamide, 31% of gabapentin, and 36% of baclofen users (p = 0.664). Complete pain relief was achieved in 36% with lacosamide, 53% with gabapentin, and 21% with baclofen (p = 0.218). The treatment discontinuation rates due to intolerance were 23% for lacosamide, 31% for gabapentin, and 21% for baclofen (p = 0.825).
Conclusion: Lacosamide may be a viable second-line treatment option for refractory trigeminal neuralgia, showing comparable outcomes to gabapentin and baclofen.
Keywords: baclofen; gabapentin; lacosamide; treatment strategies; trigeminal neuralgia.
© 2025 The Author(s). Headache: The Journal of Head and Face Pain published by Wiley Periodicals LLC on behalf of American Headache Society.
Conflict of interest statement
Figures


References
-
- Bendtsen L, Zakrzewska JM, Abbott J, et al. European academy of neurology guideline on trigeminal neuralgia. Eur J Neurol. 2019;26(6):831‐849. - PubMed
-
- Ashina S, Robertson CE, Srikiatkhachorn A, et al. Trigeminal neuralgia. Nat Rev Dis Primers. 2024;10(1):39. - PubMed
-
- Di Stefano G, De Stefano G, Leone C, et al. Real‐world effectiveness and tolerability of carbamazepine and oxcarbazepine in 354 patients with trigeminal neuralgia. Eur J Pain. 2021;25(5):1064‐1071. - PubMed
-
- Cruccu G. Trigeminal neuralgia. CONTINUUM Lifelong Learn Neurol. 2017;23(2):396‐420. http://journals.lww.com/00132979‐201704000‐00008 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
