

Post-Discharge COVID-19 Symptoms Predict 1-Year Functional Decline, Falls, and Emergency Department Visits: A Cohort Study
- PMID: 40341679
- PMCID: PMC12205281
- DOI: 10.1111/jgs.19490
Post-Discharge COVID-19 Symptoms Predict 1-Year Functional Decline, Falls, and Emergency Department Visits: A Cohort Study
Abstract
Background: Hospitalization frequently results in persistent symptoms among older adults, raising concerns about the long-term impacts of acute events-a problem amplified by COVID-19. We investigated the effects of persistent symptoms on functional decline and unplanned events over 1 year in older patients recovering from COVID-19 hospitalization.
Methods: This prospective cohort included patients aged ≥ 50 years who survived COVID-19 hospitalization between March and December 2020 as part of the CO-FRAIL study at Brazil's largest academic medical center. Persistent symptoms were defined as those reported at admission and continuously present at one-, three-, six-, nine-, and 12-month post-discharge, covering 16 symptoms. Outcomes included functional decline in basic activities of daily living (ADL), mobility activities, instrumental activities of daily living (IADL), number of falls, emergency department (ED) visits, and hospital readmissions. Associations between persistent symptoms and outcomes were examined using mixed-effects negative binomial regression models adjusted for sociodemographic, clinical, hospitalization-related factors, and post-discharge rehabilitation.
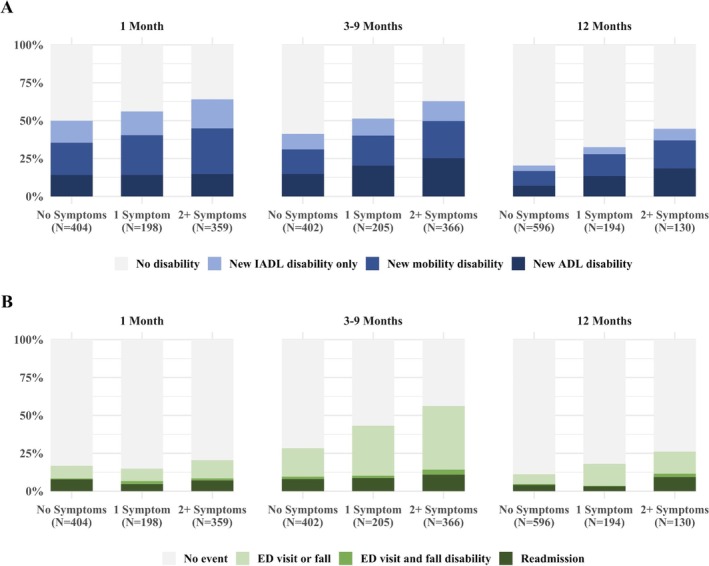
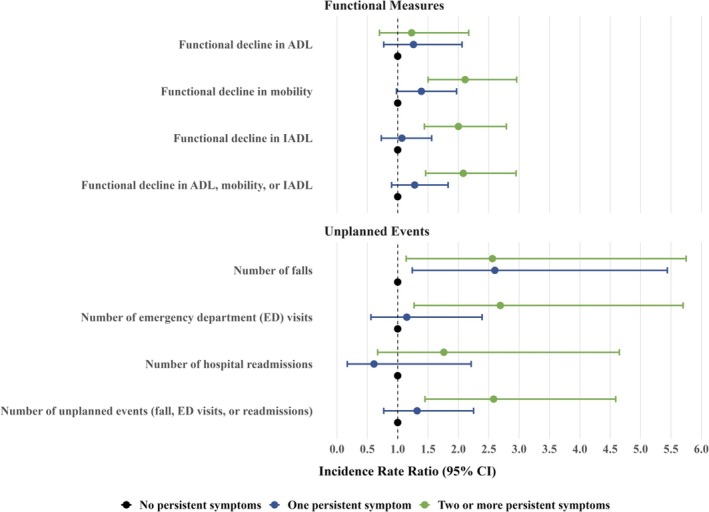
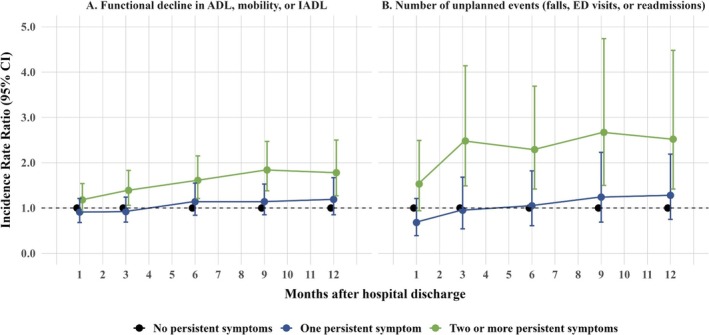
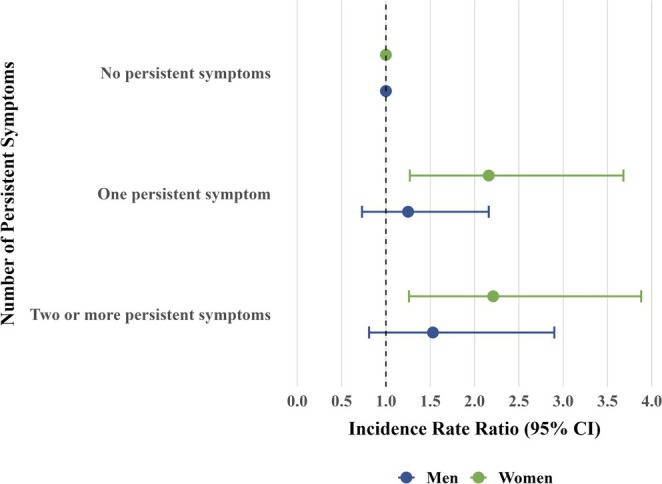
Results: Among 1019 patients (mean age = 65 ± 10 years; women = 45%; White = 62%), 324 (32%) experienced persistent symptoms throughout the year. Fatigue (28%), myalgia (19%), and dyspnea (13%) were the most common. Patients with ≥ 2 symptoms had an increased risk of functional decline in mobility activities (IRR = 2.11; 95% CI = 1.50-2.96), IADL (IRR = 2.00; 95% CI = 1.44-2.79), falls (IRR = 2.56; 95% CI = 1.14-5.75), and ED visits (IRR = 2.69; 95% CI = 1.27-5.70), but not readmissions. Among women, ≥ 1 persistent symptom was associated with a twofold increased risk of ADL decline. One year after discharge, patients with ≥ 2 persistent symptoms developed 1.27 more new disabilities (3.26 vs. 1.99 on a 15-point functional scale) and had 31 more unplanned events per 100 person-years (54.3 vs. 23.2) than those without symptoms.
Conclusions: Persistent symptoms after hospitalization are common and contribute to functional decline, falls, and ED visits in older COVID-19 survivors. These findings suggest that greater attention to symptom burden may support risk identification and improve post-discharge care planning.
Keywords: COVID‐19; functional decline; hospital; persistent symptoms; post‐acute care.
© 2025 The Author(s). Journal of the American Geriatrics Society published by Wiley Periodicals LLC on behalf of The American Geriatrics Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Arispe I. E., Gindi R. M., and Madans J. H., “Health, United States, 2019,” 2021, accessed August 31, 2024, https://www.cdc.gov/nchs/data/hus/hus19‐508.pdf.
-
- van Seben R., Covinsky K. E., Reichardt L. A., et al., “Insight Into the Posthospital Syndrome: A 3‐Month Longitudinal Follow Up on Geriatric Syndromes and Their Association With Functional Decline, Readmission, and Mortality,” Journals of Gerontology: Series A, Biological Sciences and Medical Sciences 75 (2020): 1403–1410, 10.1093/gerona/glaa039. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
