

Five year outcomes of primary and secondary Single-Anastomosis Duodeno-Ileal bypass with Sleeve gastrectomy (SADI-S)
- PMID: 40343655
- PMCID: PMC12130166
- DOI: 10.1007/s11695-025-07888-4
Five year outcomes of primary and secondary Single-Anastomosis Duodeno-Ileal bypass with Sleeve gastrectomy (SADI-S)
Abstract
Background: The single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) can be performed as a primary or (planned) secondary metabolic bariatric procedure. The aims of this study were to compare mid-term outcomes up to 5 years after primary vs secondary SADI-S and between different common channel (CC) lengths.
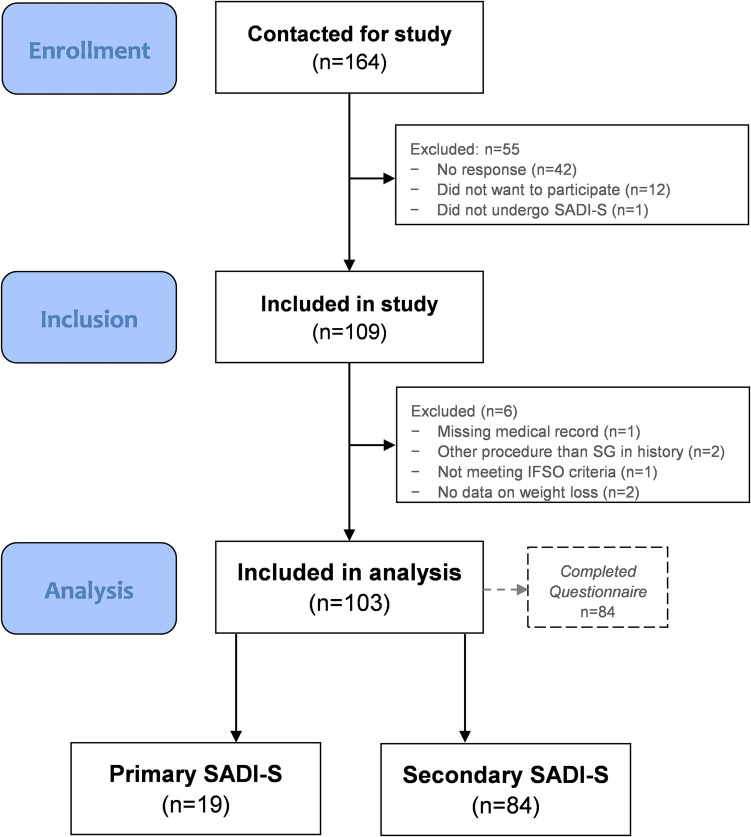
Methods: Multicenter retrospective cohort study including 103 patients who underwent SADI-S between 06-2015 and 02-2019. Outcomes on weight loss, nutrient status, health-related quality of life (HRQoL) and gastro-intestinal symptoms until 5 years postoperatively were evaluated and compared between primary (n = 19) vs secondary SADI-S (n = 84), and CC length ≤ 250 cm (n = 66,) vs > 250 cm (n = 33).
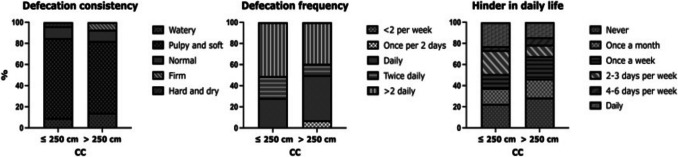
Results: Mean total weight loss (TWL) at 5 years of follow-up was higher for patients who underwent primary SADI-S compared to secondary SADI-S (34.8 (29.8-39.9)% vs 15.9 (13.0-18.9)%, p < 0.001) and for CC length ≤ 250 cm compared to > 250 cm (25.3 (21.8-28.9)% vs 21.3 (17.2-25.4)%, p = 0.12). Patients who underwent primary SADI-S also had significantly higher scores on the domains of the BODY-Q HRQoL questionnaire (p < 0.05 for all), with the exception of sexual well-being. Nutrient status and gastro-intestinal symptoms were comparable between the indication groups, but CC length ≤ 250 cm tended to result in more nutrient deficiencies and higher defecation frequency.
Conclusion: Both primary and secondary SADI-S result in durable weight loss outcomes up to 5 years postoperatively. It is imperative that CC length should be at least 250 cm to prevent malnutrition and gastro-intestinal complaints. Furthermore, focus on HRQoL is essential in future research into SADI-S.
Keywords: Conversion surgery; Recurrent weight gain; SADI-S; Secondary surgery; Single-anastomosis duodeno-ileal bypass; Sleeve gastrectomy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical Approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed Consent: Informed consent was obtained from all individual participants included in the study. Competing interests: The authors declare no competing interests
Figures



References
-
- IFSO. IFSO 8th Global Registry Report 2023. Available from: https://www.ifso.com/ifso-registry.php. Accessed 26-09-2023.
-
- Sanchez-Pernaute A, Rubio MA, Cabrerizo L, Ramos-Levi A, Perez-Aguirre E, Torres A. Single-anastomosis duodenoileal bypass with sleeve gastrectomy (SADI-S) for obese diabetic patients. Surg Obes Relat Dis. 2015;11(5):1092–8. 10.1016/j.soard.2015.01.024. - PubMed
-
- Andalib A, Alamri H, Almuhanna Y, Bouchard P, Demyttenaere S, Court O. Short-term outcomes of revisional surgery after sleeve gastrectomy: a comparative analysis of re-sleeve, Roux en-Y gastric bypass, duodenal switch (Roux en-Y and single-anastomosis). Surg Endosc. 2021;35(8):4644–52. 10.1007/s00464-020-07891-z. - PubMed
-
- Martini F, Paolino L, Marzano E, D’Agostino J, Lazzati A, Schneck AS, et al. Single-Anastomosis Pylorus-Preserving Bariatric Procedures: Review of the Literature. Obes Surg. 2016;26(10):2503–15. 10.1007/s11695-016-2310-1. - PubMed
-
- Sanchez-Pernaute A, Herrera MA, Perez-Aguirre ME, Talavera P, Cabrerizo L, Matia P, et al. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) One to three-year follow-up. Obes Surg. 2010;20(12):1720–6. 10.1007/s11695-010-0247-3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
