

Extranodal diffuse large B-cell lymphoma: Clinical and molecular insights with survival outcomes from the multicenter EXPECT study
- PMID: 40344323
- PMCID: PMC12365540
- DOI: 10.1002/cac2.70033
Extranodal diffuse large B-cell lymphoma: Clinical and molecular insights with survival outcomes from the multicenter EXPECT study
Abstract
Background: Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of aggressive non-Hodgkin's lymphoma with distinct clinical and molecular heterogeneity. DLBCL that arises in extranodal organs is particularly linked to poor prognosis. This study aimed to determine the clinical and molecular characteristics of extranodal involvement (ENI) in DLBCL and assess the actual survival status of the patients.
Methods: In this population-based cohort study, we investigated the clinical features of 5,023 patients newly diagnosed with DLBCL. Their clinical conditions, eligibility criteria, and sociodemographic details were recorded and analyzed. Gene panel sequencing was performed on 1,050 patients to discern molecular patterns according to ENI.
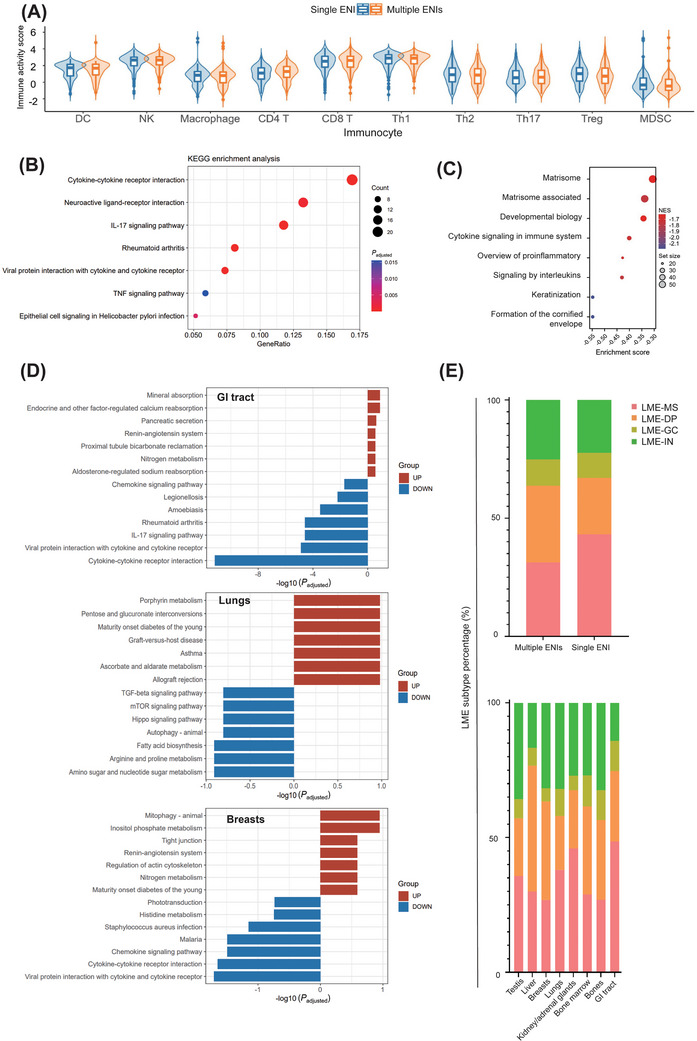
Results: The 2-year overall survival (OS) rate was 76.2% [95% confidence interval (CI), 74.0%-78.2%], and the 5-year OS rate was 67.9% (95% CI, 65.2%-70.4%). The primary treatment was immunochemotherapy with rituximab. Specific lymphoma involvement sites, especially the bones, bone marrow, and central nervous system, were identified as independent adverse prognostic factors. A high prevalence of non-germinal center B-cell (non-GCB) phenotype and myeloid differentiation primary response 88 (MYD88)/CD79B mutations were noted in lymphomas affecting the breasts, skin, uterus, and immune-privileged sites. Conversely, the thyroid and gastrointestinal tract showed a low occurrence of non-GCB phenotype. Remarkably, patients with multiple ENIs exhibited a high frequency of MYD88, tet methylcytosine dioxygenase 2 (TET2), CREB binding protein (CREBBP) mutations, increased MYD88L265P and CD79B mutation (MCD)-like subtypes, and poor prognosis. Genetic subtype-guided immunochemotherapy showed good efficacy in subgroup analyses after propensity score matching with 5-year OS and progression-free survival rates of 85.0% (95% CI, 80.6%-89.5%) and 72.1% (95% CI, 67.3%-76.7%).
Conclusions: In the rituximab era, this large-scale retrospective analysis from Asia confirmed the poor prognosis of DLBCL with multiple ENIs and underscored the efficacy of genetic subtype-guided immunochemotherapy in treating extranodal DLBCL.
Keywords: Diffuse large B‐cell lymphoma; disease progression; extranodal involvement; oncogenic mutation; prognosis; targeted therapy.
© 2025 The Author(s). Cancer Communications published by John Wiley & Sons Australia, Ltd on behalf of Sun Yat‐sen University Cancer Center.
Conflict of interest statement
We declare no competing interests.
Figures




References
-
- A clinical evaluation of the International Lymphoma Study Group classification of non‐Hodgkin's lymphoma. The Non‐Hodgkin's Lymphoma Classification Project. Blood. 1997;89(11):3909–18. - PubMed
-
- Kridel R, Telio D, Villa D, Sehn LH, Gerrie AS, Shenkier T, et al. Diffuse large B‐cell lymphoma with testicular involvement: outcome and risk of CNS relapse in the rituximab era. Br J Haematol. 2017;176(2):210–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 23J41900100/Shanghai Clinical Research Center for Cell Therapy
- 82130004/National Natural Science Foundation of China
- SHDC2020CR1032B/Clinical Research Plan of Shanghai Hospital Development Center
- 2022YFC2502600/National Key Research and Development Program
- DLY201601/Multicenter Clinical Research Project by Shanghai Jiao Tong University School of Medicine
LinkOut - more resources
Full Text Sources
