

Predictive accuracy of changes in the inferior vena cava diameter for predicting fluid responsiveness in patients with sepsis: A systematic review and meta-analysis
- PMID: 40344560
- PMCID: PMC12064207
- DOI: 10.1371/journal.pone.0310462
Predictive accuracy of changes in the inferior vena cava diameter for predicting fluid responsiveness in patients with sepsis: A systematic review and meta-analysis
Abstract
Background: Existing guidelines emphasize the importance of initial fluid resuscitation therapy in sepsis management. However, in previous meta-analyses, there have been inconsistencies in differentiating between spontaneously breathing and mechanically ventilated septic patients.
Objective: To consolidate the literature on the predictive accuracy of changes in the inferior vena cava diameter (∆IVC) for fluid responsiveness in septic patients.
Methods: The Embase, Web of Science, Cochrane Library, MEDLINE, PubMed, Wanfang, China National Knowledge Infrastructure (CNKI), Chinese Biomedical (CBM) and VIP (Weipu) databases were comprehensively searched. Statistical analyses were performed with Stata 15.0 software and Meta-DiSc 1.4.
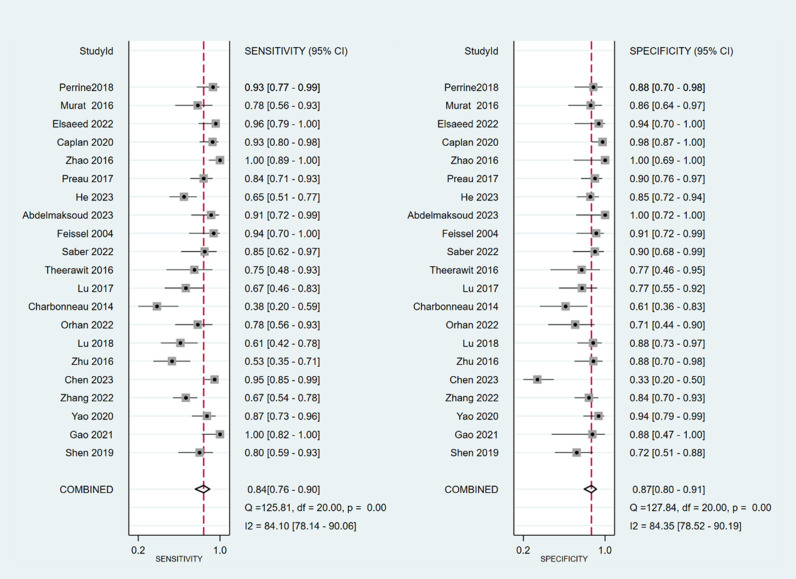
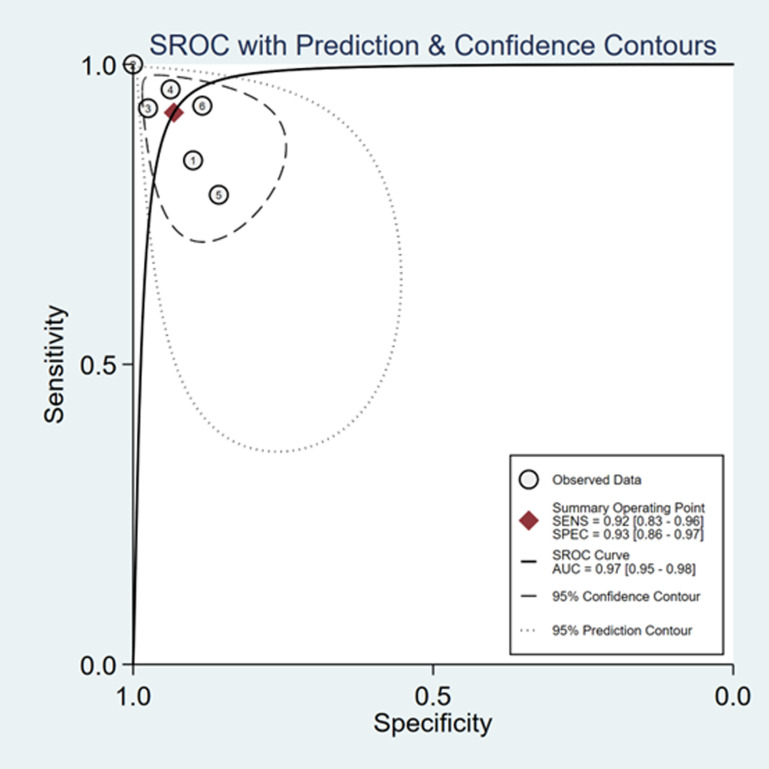
Results: Twenty-one research studies were deemed suitable for inclusion. The sensitivity and specificity of ∆ IVC were 0.84 (95% CI 0.76, 0.90) and 0.87 (95% CI 0.80, 0.91), respectively. With respect to the distensibility of the inferior vena cava (dIVC), the sensitivity was 0.79 (95% CI 0.68, 0.86), and the specificity was 0.82 (95% CI 0.73, 0.89). For collapsibility of the inferior vena cava (cIVC), the sensitivity and specificity values were 0.92 (95% CI 0.83, 0.96) and 0.93 (95% CI 0.86, 0.97), respectively.
Conclusion: The results indicated that ∆IVC is as a dependable marker for fluid responsiveness in sepsis patients. dIVC and cIVC also exhibited high levels of accuracy in predicting fluid responsiveness in septic patients.
Copyright: © 2025 Zhang et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




















Similar articles
-
Accuracy of indices of inferior vena cava in predicting fluid responsiveness in patients with shock: A systematic review and meta-analysis.Intensive Crit Care Nurs. 2025 Aug;89:104015. doi: 10.1016/j.iccn.2025.104015. Epub 2025 Apr 8. Intensive Crit Care Nurs. 2025. PMID: 40187099
-
Ultrasonographic measurement of the respiratory variation in the inferior vena cava diameter is predictive of fluid responsiveness in critically ill patients: systematic review and meta-analysis.Ultrasound Med Biol. 2014 May;40(5):845-53. doi: 10.1016/j.ultrasmedbio.2013.12.010. Epub 2014 Feb 2. Ultrasound Med Biol. 2014. PMID: 24495437
-
Does Respiratory Variation in Inferior Vena Cava Diameter Predict Fluid Responsiveness: A Systematic Review and Meta-Analysis.Shock. 2017 May;47(5):550-559. doi: 10.1097/SHK.0000000000000801. Shock. 2017. PMID: 28410544
-
Agreement between subcostal and transhepatic longitudinal imaging of the inferior vena cava for the evaluation of fluid responsiveness: A systematic review.J Crit Care. 2022 Oct;71:154108. doi: 10.1016/j.jcrc.2022.154108. Epub 2022 Jul 5. J Crit Care. 2022. PMID: 35797826
-
The ultrasonographic evaluation of caudal vena cava diameter before and after fluid replacement in neonatal dehydrated calves with diarrhea.BMC Vet Res. 2025 Jul 2;21(1):424. doi: 10.1186/s12917-025-04759-z. BMC Vet Res. 2025. PMID: 40604891 Free PMC article.
References
-
- Xie J, Wang H, Kang Y, Zhou L, Liu Z, Qin B, et al.. The epidemiology of sepsis in Chinese ICUs: a national cross-sectional survey. Critical Care Medicine. 2019;48(3):e209-e218. - PubMed
-
- Tiru B, DiNino EK, Orenstein A, Mailloux PT, Pesaturo A, Gupta A, et al.. The Economic and Humanistic Burden of Severe Sepsis. Pharmacoeconomics, 2015,33(9):925-937. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
