

Lymphatic Abnormalities in Fontan: Case Report of Plastic Bronchitis
- PMID: 40345728
- PMCID: PMC12245420
- DOI: 10.1016/j.jaccas.2025.103283
Lymphatic Abnormalities in Fontan: Case Report of Plastic Bronchitis
Abstract
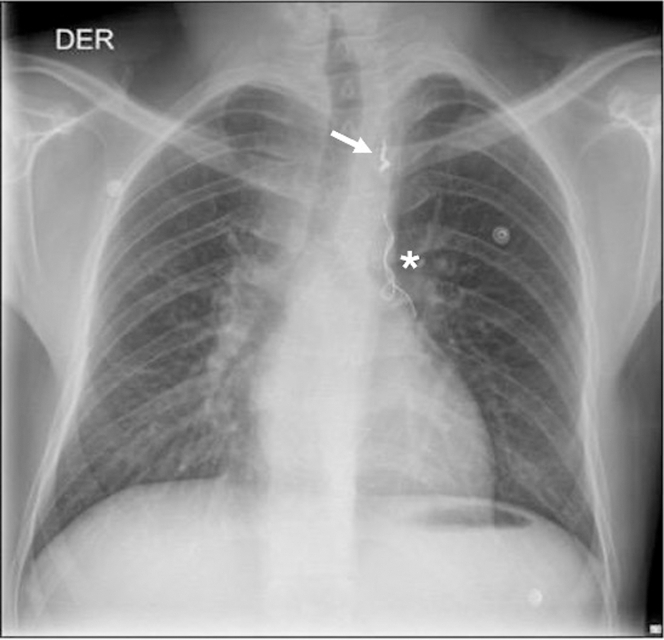
Plastic bronchitis is a rare but severe complication in Fontan patients. Central lymphatic evaluation may direct therapy for these complications. We present a 22-year-old mn post-Fontan who presented with bronchial casts. Initial medical management failed to reduce cast formation. Dynamic contrast-enhanced magnetic resonance lymphangiography was conducted for targeted management, revealing an aberrant lymphatic channel draining to the right pulmonary hilum. After 2 failed attempts, a percutaneous intervention with a proctoring aid resolved symptoms, improving the patient's condition. This case contributes to the literature on the role of central lymphatic imaging in diagnosing and treating lymphatic complications in Fontan patients. However, expertise is needed to successfully deliver targeted interventional lymphatic therapy. Understanding the management of Fontan patients requires recognizing lymphatic complications. Studying the central lymphatic system through dynamic contrast-enhanced magnetic resonance lymphangiography in patients with Fontan aids in diagnosing lymphatic abnormalities and targeting treatment.
Keywords: Fontan palliation; congenital heart disease; lymphatic abnormalities; magnetic resonance lymphangiogram; plastic bronchitis; therapeutic embolization.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures






References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
