

Outcomes of elderly patients with relapsed refractory multiple myeloma (RRMM) treated with teclistamab: a multicenter study from the U.S. Multiple Myeloma Immunotherapy Consortium
- PMID: 40346049
- PMCID: PMC12064690
- DOI: 10.1038/s41408-025-01297-7
Outcomes of elderly patients with relapsed refractory multiple myeloma (RRMM) treated with teclistamab: a multicenter study from the U.S. Multiple Myeloma Immunotherapy Consortium
Abstract
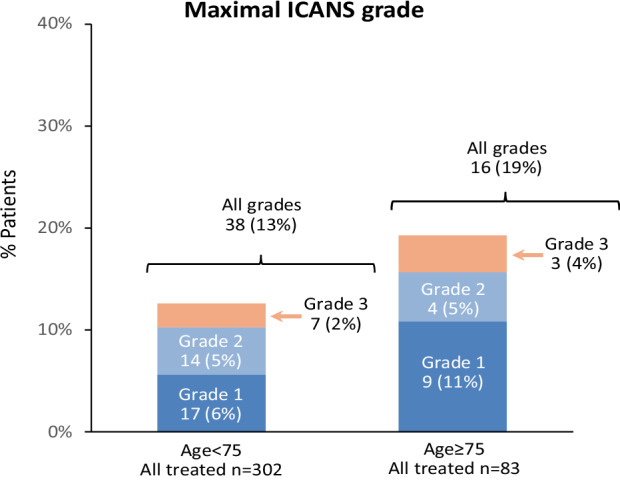
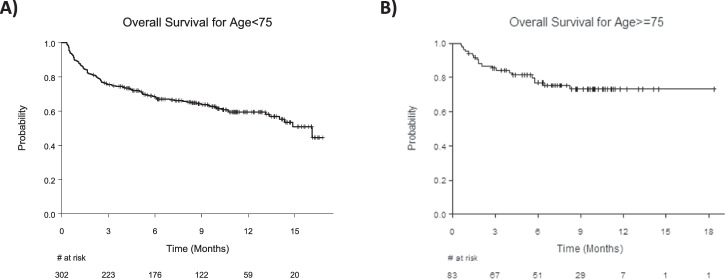
Teclistamab, a BCMA-directed bispecific antibody, received regulatory approval for relapsed/refractory multiple myeloma (RRMM) based on the MajesTEC-1 study. Despite the fact that myeloma is primarily a cancer of elderly adults, only 15% of MajesTEC-1 participants (n = 24) were ≥75 years old. In this multicenter retrospective study, we report real-world outcomes of a large cohort of older RRMM patients treated with teclistamab. Of 385 analyzed patients, 83 (22%) were in the older group (age ≥75) and 302 (78%) in the younger group (age <75). Compared to the younger group, the older group had less adverse baseline disease characteristics, including a lower incidence of high-risk cytogenetics (44.6% vs. 57.9%, p = 0.03) and extramedullary disease (22% vs. 40%, p = 0.02). There were no significant differences in rates of any-grade CRS (52% vs. 59%, p = 0.27), any-grade ICANS (19% vs. 13%, p = 0.12), and overall response rate (62% vs. 53%, p = 0.17) between the older and younger groups. In multivariable analysis, age was not significantly associated with survival outcomes. Our findings suggest that teclistamab is safe and efficacious in well-selected patients ≥75 years old, and advanced age alone should not preclude teclistamab administration.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: JAD reports consulting: Janssen; speakers’ bureau: Janssen. AA reports research funding from AbbVie, Adaptive Biotech, K36-therapeutics, J&J, Regeneron Pharmaceuticals; advisory role for Karyopharm, BMC, Sanofi, J&J, Pfizer. RB reports consulting: Adaptive Biotech, BMS, Caribou Biosciences, Genentech, Janssen, Karyopharm, Legend Biotech, Pfizer, Sanofi, SparkCures; Research: AbbVie, BMS, Janssen, Novartis, Pack Health, Prothena, Sanofi. JK reports consulting: GPCR, Janssen, Prothena, Legend Biotech; research: Prothena, Ascentage, Janssen, Karyopharm, GPCR. MRG reports consulting or advisory role - Bristol Myers Squibb and Arcellx. KJ reports being an advisory board consultant for Janssen, Pfizer, and BioLineRx. LS reports consulting: BMS. SSA reports consulting: Sanofi. HH reports consulting: Janssen; speaker bureaus: Janssen, Karyopharm. LM reports advisory board with legend and bioline Rx. GK reports consulting: BMS, Arcellx, Sanofi, Janssen, Cellectar, Pfizer, Kedrion; Research: BMS, Janssen, AbbVie. YL reports consulting: Janssen, Legend, Celgene, Sanofi, BMS, Pfizer, Regeneron, Genentech, NexImmune, Caribou; research funding: Janssen, Celgene, BMS. JM reports consulting: Envision, Novartis, Caribou Bio, Sana Technologies, Legend Biotech, Cargo Therapeutics. Ad Board: Autolus. Consulting/Ad board: Kite/scimentum, Allovir, BMS, CRISPR, Nektar. DS reports consulting for BMS, GSK, Sanofi, Janssen, Opna Bio, Genentech, Pfizer, and AbbVie. FA reports serving as advisor and speaker for Bristol Myers Squibb, Celgene, Caribou Biosciences; received research funding from Allogene Therapeutics, Celgene, GlaxoSmithKline, Bristol Myers Squibb, and Caribou Biosciences. ALG reports research funding from Johnson & Johnson, Novartis, CRISPR Therapeutics, and Tmunity Therapeutics; consultant relationships with Gracell, Johnson & Johnson, Smart Immune, AbbVie, Regeneron, Bristol Myers Squibb, and Novartis; Independent Data Monitoring Committee service for Johnson & Johnson. SS reports research: Magenta Therapeutics, BMS, Allogene, Janssen, Novartis, AbbVie; Advisory Board/Consultancy: BMS, Janssen, Sanofi, Oncopeptides, Takeda, Regeneron, AbbVie, Pfizer, BiolineRx, Legend, Kite. AJC reports research funding: Janssen, BMS, Juno/Celgene, Sanofi, Regeneron, IGM BIosciences, Nektar, Harpoon, Adaptive Biotechnologies, Caelum, AbbVie, OpnaBio, Karyopharm, Advisory/Consulting: Sebia, Janssen, BMS, Sanofi, HopeAI, Adaptive Biotechnologies, Pfizer. LDA reports consulting: Janssen, Celgene, BMS, Amgen, GSK, AbbVie, BeiGene, Cellectar, Sanofi, Prothena. Research: BMS, Celgene, GSK, Janssen, AbbVie. DKH reports research funding from Bristol Myers Squibb, Janssen, Karyopharm, Kite Pharma, and Adaptive Biotech; Consulting or advisory role for Bristol Myers Squibb, Janssen, Legend Biotech, Pfizer, Kite Pharma, AstraZeneca, and Karyopharm. ShRi reports honoraria: Janssen, BMS, Genentech, Karyopharm Therapeutics, MJH LifeSciences; steering committees: Gracell Therapeutics, BMS; research support: Janssen, BMS, C4 Therapeutics, Gracell Therapeutics, Heidelberg Pharma; consulting: Genentech, Janssen, BMS, Karyopharm Therapeutics. KKP reports consulting: BMS, Janssen, AstraZeneca, Legend Biotech, Kite, Genentech, AbbVie, Sanofi, Caribou, Takeda, Regeneron, Poseida. HCL reports consulting: Bristol Myers Squibb, Pfizer, Janssen, Regeneron, GlaxoSmithKline, Sanofi, AbbVie, Takeda Pharmaceuticals, Allogene Therapeutics, Menarini, Alexion Pharmaceuticals; research funding: Amgen, Bristol Myers Squibb, Janssen, GSK, Regeneron, Takeda Pharmaceuticals. AGC reports Janssen: speaker bureau, advisory board, research funding; Sanofi: advisory board, speaker bureau; BMS: advisory board; Pfizer: advisory board, speaker bureau; Cellectar: advisory board; Amgen: speaker bureau. The remaining authors have no conflicts to disclose. Ethics approval and consent to participate: All patients included in this analysis have provided informed consent for participation in the study. The study was conducted in compliance with the International Conference on Harmonization (ICH) and Good Clinical Practices (GCPs). The protocol was approved by the respective Institutional Review Board or ethics committee at each of the participating institutions (MD Anderson Cancer Center, Houston, TX; Fred Hutchinson Cancer Center, Seattle, WA; Cleveland Clinic Lerner College of Medicine, Case Western Reserve University School of Medicine, Cleveland, OH; Medical University of South Carolina, Charleston, SC; Myeloma, Waldenstrom’s, and Amyloidosis Program, Simmons Comprehensive Cancer Center, UT Southwestern Medical Center, Dallas, TX; Moffitt Cancer Center, Tampa, FL; Mount Sinai School of Medicine, New York, NY; Stanford University, Palo Alto, CA; Huntsman Cancer Institute, University of Utah, Salt Lake City, UT; Atrium Health Levine Cancer Institute, Wake Forest University School of Medicine, Charlotte, NC; University of Kansas Medical Center, Kansas City, KS; Abramson Cancer Center and Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA; Roswell Park Comprehensive Cancer Center, Buffalo, NY; Duke University Cancer Institute, Durham, NC; Mayo Clinic, Division of Hematology, Rochester, MN; Dana-Farber Cancer Institute, Boston, MA; all in the USA). All subjects provided documented informed consent. All methods were performed in accordance with the relevant guidelines and regulations. All authors had access to the data and contributed to the analysis and interpretation of the results. The authors confirm the accuracy and completeness of the data.
Figures



References
-
- National Cancer Institute. Surveillance E, and End Results (SEER) Program. Cancer Stat Facts: Myeloma 2022. Available from: https://seer.cancer.gov/statfacts/html/mulmy.html.
-
- Donk, NWCJvd, Moreau P, Garfall AL, Bhutani M, Oriol A, Nooka AK, et al. Long-term follow-up from MajesTEC-1 of teclistamab, a B-cell maturation antigen (BCMA) x CD3 bispecific antibody, in patients with relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. 2023;41:8011 - DOI
Publication types
MeSH terms
Substances
Grants and funding
- P30 CA016672/CA/NCI NIH HHS/United States
- R01 CA281756/CA/NCI NIH HHS/United States
- NCI Grant P30 CA016672/U.S. Department of Health & Human Services | NIH | National Cancer Institute (NCI)
- NCI (R01CA281756-01A1)/U.S. Department of Health & Human Services | NIH | NIH Clinical Center (Clinical Center)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
