

Wearable sleep recording augmented by artificial intelligence for Alzheimer's disease screening
- PMID: 40346113
- PMCID: PMC12064732
- DOI: 10.1038/s41514-025-00219-y
Wearable sleep recording augmented by artificial intelligence for Alzheimer's disease screening
Abstract
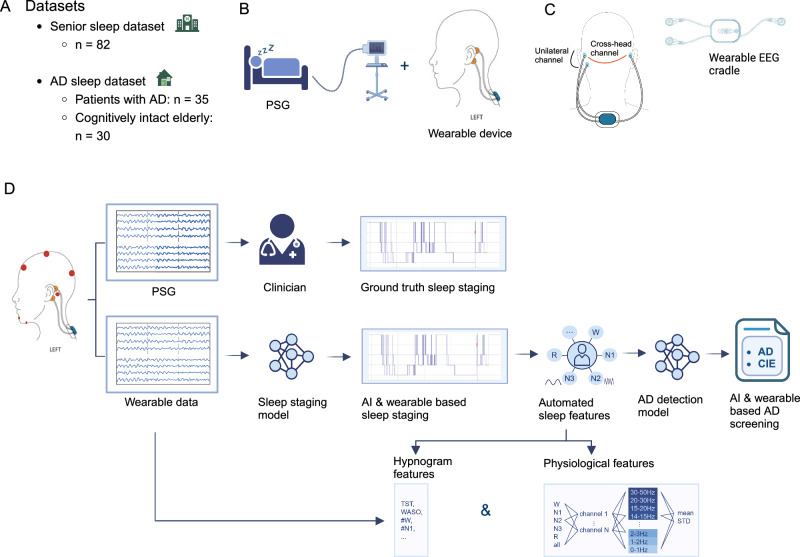
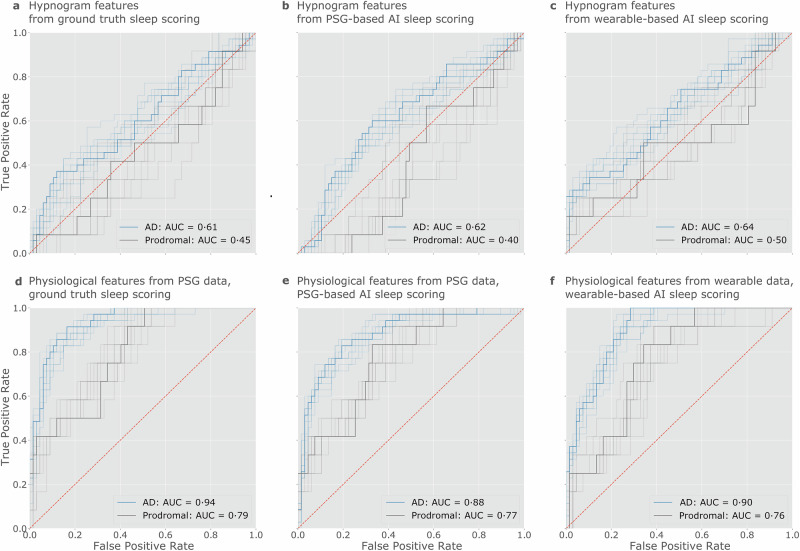
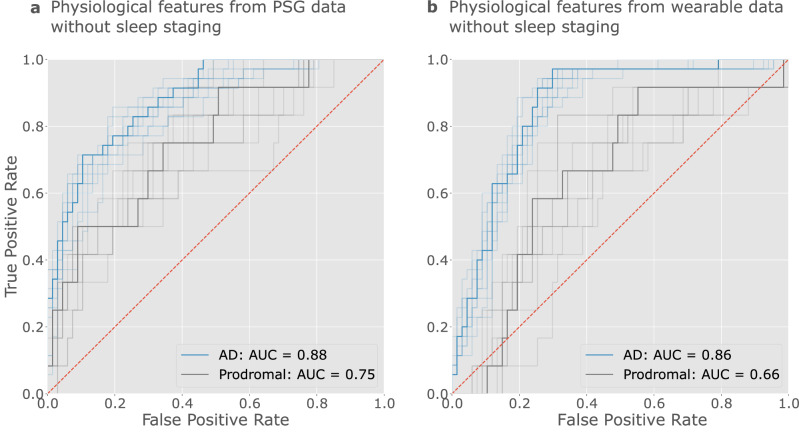
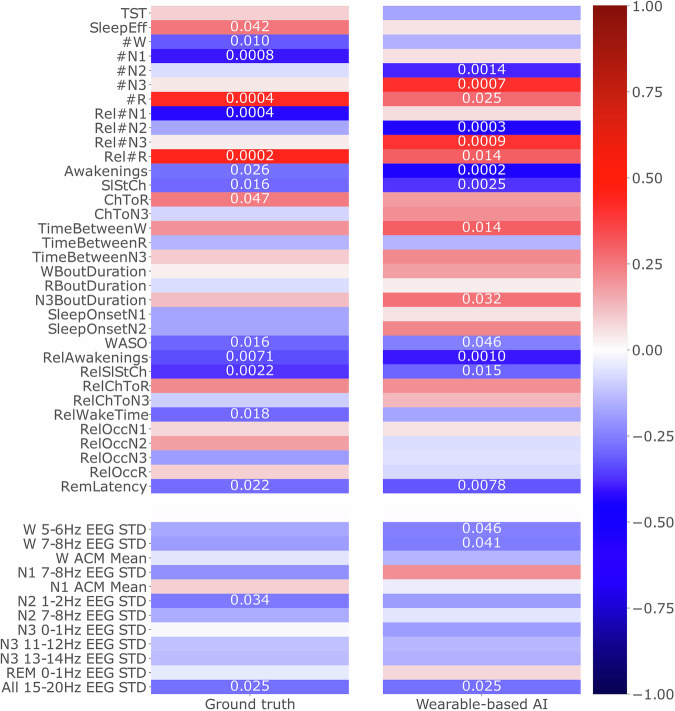
The recent emergence of wearable devices will enable large scale remote brain monitoring. This study investigated whether multimodal wearable sleep recordings could help screening for Alzheimer's disease (AD). Measurements were acquired simultaneously from polysomnography and a wearable device, measuring electroencephalography (EEG) and accelerometry (ACM) in 67 elderly without cognitive symptoms and 35 AD patients. Sleep staging was performed using an AI model (SeqSleepNet), followed by feature extraction from hypnograms and physiological signals. Using these features, a multi-layer perceptron was trained for AD detection, with elastic net identifying key features. The wearable AD detection model achieved an accuracy of 0.90 (0.76 for prodromal AD). Single-channel EEG and ACM physiological features captured sufficient information for AD detection and outperformed the hypnogram features, highlighting these physiological features as promising discriminative markers for AD. We conclude that wearable sleep monitoring augmented by AI shows promise towards non-invasive screening for AD in the older population.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests. Ethical approval: Studies were conducted in accordance with the Declaration of Helsinki and approved by the Ethical Committee of University Hospitals Leuven. Informed consent was obtained from all participants or their caregiver. The clinical trial numbers were NCT04755504 (S64190/B3222020000148), NCT03617497 (S61745) respectively.
Figures

References
-
- Georges J., Miller O. & Bintener, C. Dementia in Europe Yearbook 2019: Estimating The Prevalence Of Dementia In Europe, accessed 17 Apr 2024. https://www.researchgate.net/publication/339401240_Estimating_the_preval... (Alzheimer Europe, 2020).
Grants and funding
LinkOut - more resources
Full Text Sources
