

Partial arterial carbon dioxide and oxygen pressure in patients with cardiogenic shock
- PMID: 40346435
- PMCID: PMC12130108
- DOI: 10.1007/s11739-025-03926-2
Partial arterial carbon dioxide and oxygen pressure in patients with cardiogenic shock
Abstract
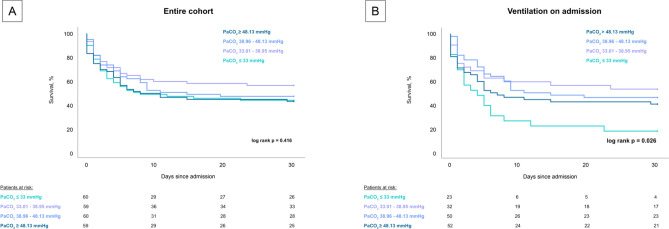
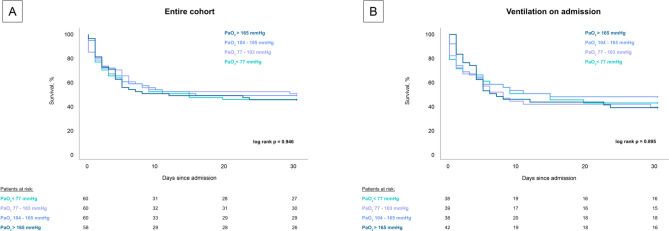
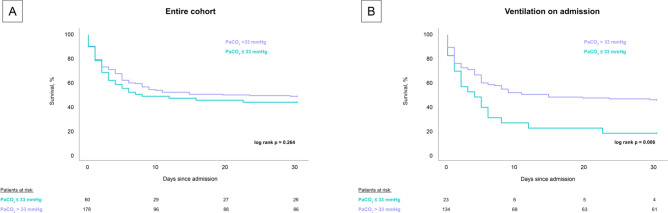
In patients with acute cardiovascular diseases, hypocapnia, hypoxia and hyperoxia are known to be associated with increased mortality. This monocentric prospective registry study included 238 consecutive patients with cardiogenic shock (CS). The study aimed to assess the prognostic impact of partial arterial carbon dioxide (PaCO2) and oxygen pressure (PaO2) on 30-day all-cause mortality. Statistical analyses included t-tests, Spearman´s correlation, Kaplan-Meier and Cox regression analyses. No difference was found between quartiles of PaCO2 (log-rank p = 0.416) and PaO2 (log-rank p = 0.946) in the entire cohort. In the subgroup of patients with ventilation on admission, patients with PaCO2 ≤ 33 mmHg showed the highest 30-day all-cause mortality compared to the other quartiles (82.6% vs. 46.9% vs. 54.0% vs. 59.6% log-rank p = 0.026). No differences were found between levels of PaO2, when stratified by quartiles (log-rank p = 0.895). After differentiation between patients with PaCO2 ≤ 33 mmHg and PaCO2 > 33 mmHg the association with 30-day all-cause mortality remained significant (82.6% vs. 54.5% log-rank p = 0.006) in ventilated patients, whereas still no difference could be seen in the entire cohort (log-rank p = 0.264). Even after multivariable adjustment PaCO2 ≤ 33 mmHg remained an independent risk factor for 30-day all-cause mortality (HR 1.936; 95% CI 1.131-3.316; p = 0.016) in ventilated CS-patients. In conclusion, no association was found between different levels of PaCO2 and PaO2 with 30-day all-cause mortality in patients with CS. However, in the subgroup of CS-patients requiring ventilation, PaCO2 ≤ 33 mmHg was associated with an increased 30-day all-cause mortality.
Keywords: Carbon dioxide; Cardiogenic shock; Mortality; Oxygen; Ventilation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare that they have no conflict of interest. Ethics approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the medical ethics committee II of the Medical Faculty Mannheim, University of Heidelberg. Consent to participate: Informed consent was waived by the medical ethics committee II of the Medical Faculty Mannheim, University of Heidelberg.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
