

Appropriate treatment for nail breakage following femur intertrochanteric fractures without additional reduction: case series and literature review
- PMID: 40346578
- PMCID: PMC12063332
- DOI: 10.1186/s12891-025-08669-x
Appropriate treatment for nail breakage following femur intertrochanteric fractures without additional reduction: case series and literature review
Abstract
Background: Intramedullary nail breakage is an uncommon complication in patients with femoral intertrochanteric fractures treated with proximal femoral nail antirotation. Salvage surgery for nail breakages associated with delayed union or nonunion is challenging, particularly when breakage occurs within an acceptable reduction range, complicating implant selection. This study evaluated outcomes in patients with proximal femoral nail antirotation breakage, acceptable reduction, and fixation treated with the long proximal femoral nail antirotation change with distal screw dynamization and lateral cortical notching procedure.
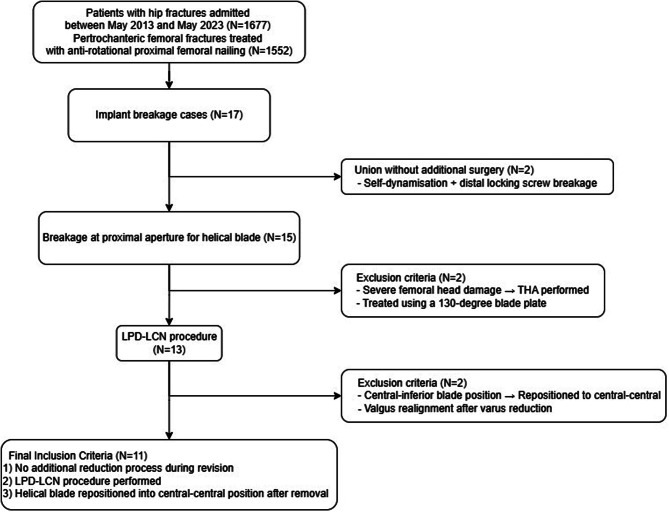
Methods: Eleven patients who underwent the long proximal femoral nail antirotation change with distal screw dynamization and lateral cortical notching procedure between May 2013 and May 2023 with no additional fracture reduction required during salvage surgery and with a helical blade screw resinserted at the same position after removal were observed for > 1 year.
Results: The average time to full weight-bearing was 8.44 ± 0.82 weeks (mean ± standard deviation) and to return to normal activities was 18.05 ± 0.89 weeks. The Harris Hip Score was 78.64 ± 1.03 at 12 months; all patients resumed independent walking at the final follow-up. The average fracture union time was 21.49 ± 1.75 weeks. In seven cases with a fracture gap at the time of breakage, significant change was observed in the tip-apex distance (P = 0.016) or lateral extension of the proximal femoral nail antirotation blade (P = 0.005) between the immediate post-surgery and final follow-up results, with the gap healing radiographically at 21.50 ± 1.65 weeks.
Conclusion: Patients with high functional demands, good femoral head bone stock, no acetabular disease, and isolated nail breakage due to nonunion or delayed union in the intertrochanteric area treated with proximal femoral nail antirotation are suitable candidates for osteosynthesis. When reduction is within an acceptable range and the lag screw is centrally placed, long proximal femoral nail antirotation with lateral notching and dynamization offers a minimally invasive approach that reduces soft tissue injury and can yield successful outcomes.
Clinical trial number: Not applicable.
Keywords: Bone screws; Femur head; Fracture fixation; Internal hip fractures.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The protocol of this study was approved by Gwangju Veterans Hospital Institutional Review Board (no. 2024-2-1). All data were anonymized, and the requirement for informed consent was waived by the Institutional Review Board due to the retrospective nature of the study design. This research was conducted in accordance with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Karapinar L, Kumbaraci M, Kaya A, Imerci A, Incesu M. Proximal femoral nail anti-rotation (PFNA) to treat peritrochanteric fractures in elderly patients. Eur J Orthop Surg Traumatol. 2012;22:237–43. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
