

Clinicopathological Correlates of Hormone Expression-Based Subtypes of Non-Functioning Duodenal/Ampullary Neuroendocrine Tumors: A Multicenter Study of 151 Cases
- PMID: 40347392
- PMCID: PMC12065733
- DOI: 10.1007/s12022-025-09861-4
Clinicopathological Correlates of Hormone Expression-Based Subtypes of Non-Functioning Duodenal/Ampullary Neuroendocrine Tumors: A Multicenter Study of 151 Cases
Abstract
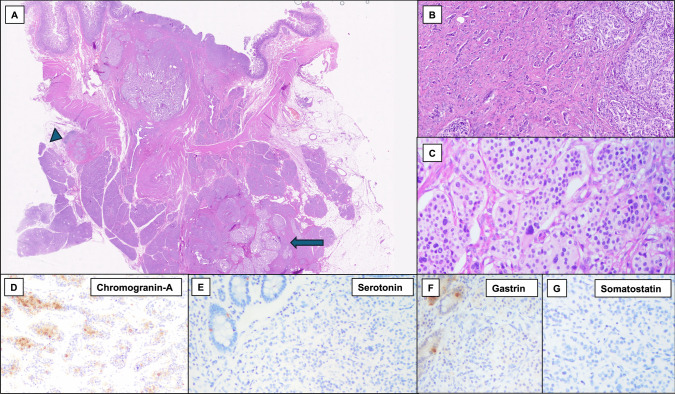
Duodenal neuroendocrine tumors (Duo-NETs) may arise in the ampullary and non-ampullary duodenum. Non-functioning Duo-NETs (NF-Duo-NETs), which account for most cases, may express various hormones. Previous studies have suggested that hormone production might be associated with biological aggressiveness. Current treatment protocols are based on functionality, tumor size, and location, but small NF-Duo-NETs may also have metastatic potential. We aimed to investigate whether tumor cell subtyping, based on hormone expression, could provide further insights into NF-Duo-NET biological behavior. We analyzed the clinico-pathological correlates of hormone expression in a multicenter series of 151 NF-Duo-NETs, subdividing tumors into five subtypes: gastrin-producing G-cell NETs (Gas-NETs), somatostatin-producing D-cell NETs (Som-NETs), serotonin-producing enterochromaffin-cell NETs (Ser-NETs), plurihormonal NETs, and gastrin-, somatostatin-, and serotonin-negative NETs (GSSN-NETs). Som-NETs were the most frequent (31%), followed by plurihormonal NETs (26%), Gas-NETs (24%), GSSN-NETs (13%), and Ser-NETs (4%). Som-NETs and GSSN-NETs were more commonly located in the ampullary region and showed significantly larger size, more frequent lymphatic and/or vascular invasion, and higher pT, pN, and American Joint Committee on Cancer (AJCC-9th edition) stages compared to Gas-NETs, which were often (77%) diagnosed at AJCC stage I. Ampullary Som-NETs showed a more invasive and metastatic potential compared to non-ampullary Som-NETs, while, among plurihormonal NETs, the predominantly expressed hormone influenced tumor biological features, with gastrin-predominant NETs showing less invasive potential. At logistic regression, both tumor cell subtype and tumor size were independently associated with aggressiveness (pT3, pN1, or pM1 stage at diagnosis). Hormonal expression profiling may be clinically relevant in NF-Duo-NETs, independently of tumor size.
Keywords: Cell subtyping; Gastrin; Null-cell tumors; Plurihormonal tumors; Somatostatin.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics Approval: Ethics approval is obtained from Pavia Ethical Committee. Consent for Publication: All authors consent to publication. Competing Interests: The authors declare no competing interests.
Figures




References
-
- Jensen RT, Rindi G, Arnold R, Lopes JM, Brandi ML, Bechstein WO, Christ E, Taal BG, Knigge U, Ahlman H, Kwekkeboom DJ, O'Toole D; Frascati Consensus Conference; European Neuroendocrine Tumor Society. Well-differentiated duodenal tumor/carcinoma (excluding gastrinomas). Neuroendocrinology. 2006;84(3):165–72. 10.1159/000098008. Epub 2007 Feb 20. PMID: 17312376. - PubMed
-
- Masui T, Ito T, Komoto I, Uemoto S; JNETS Project Study Group. Recent epidemiology of patients with gastro-entero-pancreatic neuroendocrine neoplasms (GEP-NEN) in Japan: a population-based study. BMC Cancer. 2020 Nov 14;20(1):1104. 10.1186/s12885-020-07581-y. PMID: 33189127; PMCID: PMC7666508. - PMC - PubMed
-
- Fitzgerald TL, Dennis SO, Kachare SD, Vohra NA, Zervos EE. Increasing incidence of duodenal neuroendocrine tumors: Incidental discovery of indolent disease? Surgery. 2015 Aug;158(2):466-71. 10.1016/j.surg.2015.03.042. Epub 2015 May 23. PMID: 26013986. - PubMed
-
- WHO Classification of Tumours Editorial Board. Endocrine and neuroendocrine tumours. Lyon (France): International Agency for Research on Cancer; 2022. (WHO classification of tumours series, 5th ed.; vol. 10). https://publications.iarc.fr.
-
- Vanoli A, La Rosa S, Klersy C, Grillo F, Albarello L, Inzani F, Maragliano R, Manca R, Luinetti O, Milione M, Doglioni C, Rindi G, Capella C, Solcia E. Four Neuroendocrine Tumor Types and Neuroendocrine Carcinoma of the Duodenum: Analysis of 203 Cases. Neuroendocrinology. 2017;104(2):112-125. 10.1159/000444803. Epub 2016 Feb 25. PMID: 26910321. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
