

SCORT-Cas13d Nanotherapy Precisely Targets the 'Undruggable' Transcription Factor HoxB13 in Metastatic Prostate Cancer In Vivo
- PMID: 40349174
- PMCID: PMC12199340
- DOI: 10.1002/advs.202417605
SCORT-Cas13d Nanotherapy Precisely Targets the 'Undruggable' Transcription Factor HoxB13 in Metastatic Prostate Cancer In Vivo
Abstract
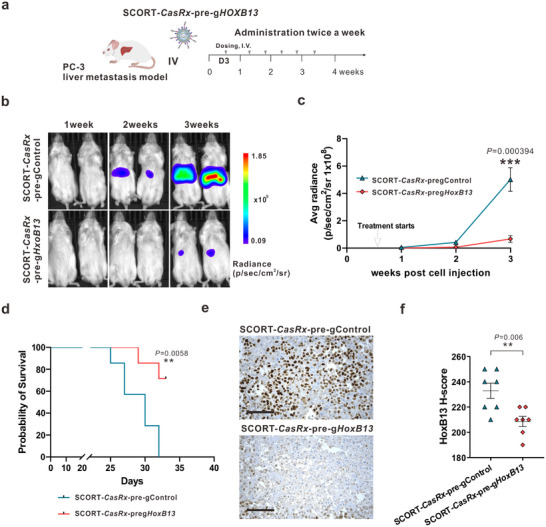
Metastatic cancer, the primary cause of cancer mortality, frequently exhibits heightened dependence on certain transcription factors (TFs), which serve as master regulators of oncogenic signaling yet are often untargetable by small molecules. Selective Cell in ORgan Targeting (SCORT) nanoparticles are developed for precise CRISPR/Cas13d mRNA and gRNA delivery to metastatic cancer cells in vivo, aiming to knock down the undruggable oncogenic TF HoxB13. In prostate cancer liver metastasis models driven by HoxB13, repeated systemic SCORT-Cas13d-gHoxB13 treatment significantly decreases HoxB13 expression, reduces metastasis, and extends mouse survival. Prolonged treatment shows no significant impact on major organ function, histology or immune markers. Mechanistically, SCORT-Cas13d-gHoxB13 treatment suppresses metastatic tumor proliferation and angiogenesis while promoting apoptosis by regulating multiple gene pathways. Unexpectedly, it inhibits the non-canonical, EMT-independent oncogenic function of Snail. These findings suggest that SCORT-Cas13d-gHoxB13 can effectively and safely target the undruggable HoxB13 in metastatic prostate cancer, positioning CRISPR/Cas13d as a potential treatment.
Keywords: HoxB13; SCORT nanoparticles; SCORT‐Cas13d nanotherapy; mechanistic insights into therapeutic action; metastatic prostate cancer; undruggable oncogenic transcription factors.
© 2025 The Author(s). Advanced Science published by Wiley‐VCH GmbH.
Conflict of interest statement
Q.W., Z.C., and Y.D. are inventors on a patent filed by Duke University that relates to the research reported in this paper. J.H. is a consultant for or owns shares in the following companies: Kingmed, MoreHealth, OptraScan, Genetron, Omnitura, Vetonco, York Biotechnology, Genecode, VIVA Biotech, and Sisu Pharma, and received grants from Zenith Epigenetics, BioXcel Therapeutics, Inc., and Fortis Therapeutics.
Figures






References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous