

Development and Validation of a Novel Nomogram Risk Prediction Model for In-Hospital Death Following Extended Aortic Arch Repair for Acute Type A Aortic Dissection
- PMID: 40351672
- PMCID: PMC12059769
- DOI: 10.31083/RCM26943
Development and Validation of a Novel Nomogram Risk Prediction Model for In-Hospital Death Following Extended Aortic Arch Repair for Acute Type A Aortic Dissection
Abstract
Background: Extended aortic arch repair (EAR) is increasingly adopted for treating acute type A aortic dissection (ATAAD). However, existing prediction models may not be suitable for assessing the in-hospital death risk in ATAAD patients undergoing EAR. This study aims to develop a comprehensive risk prediction model for in-hospital death following EAR based on patient's preoperative status and surgical data, which may contribute to identification of high-risk individuals and improve outcomes following EAR.
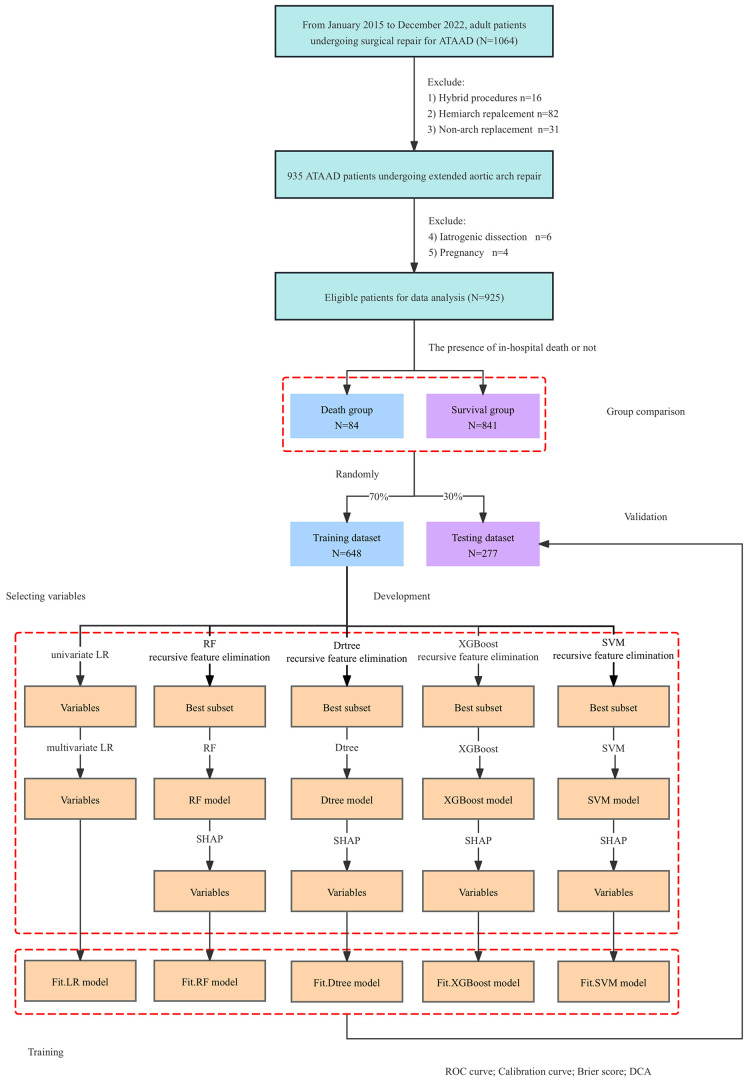
Methods: We reviewed clinical records of consecutive adult ATAAD patients undergoing EAR at our institute between January 2015 and December 2022. Utilizing data from 925 ATAAD patients undergoing EAR, we employed multivariable logistic regression and machine learning techniques, respectively, to develop nomograms for in-hospital mortality. Employed machine learning techniques included simple decision tree, random forest (RF), eXtreme Gradient Boosting (XGBoost), and support vector machine (SVM).
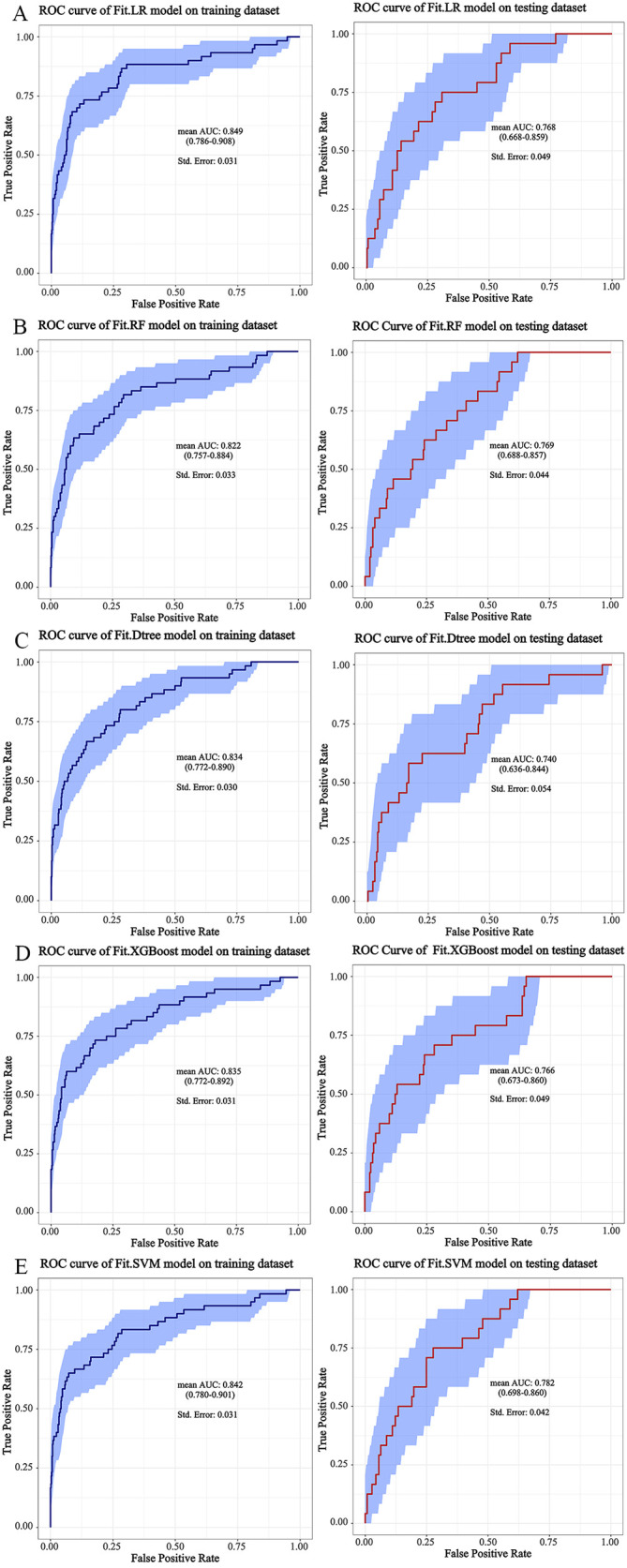
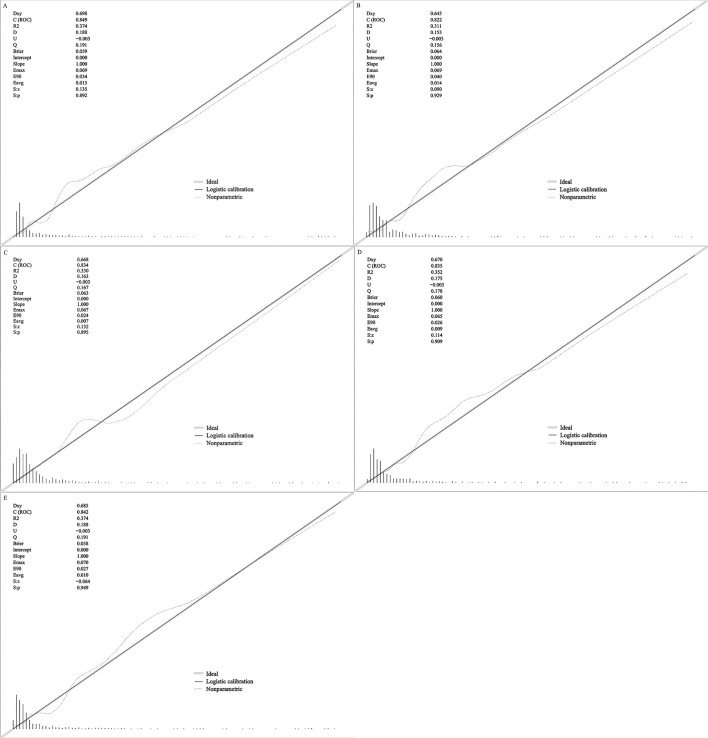
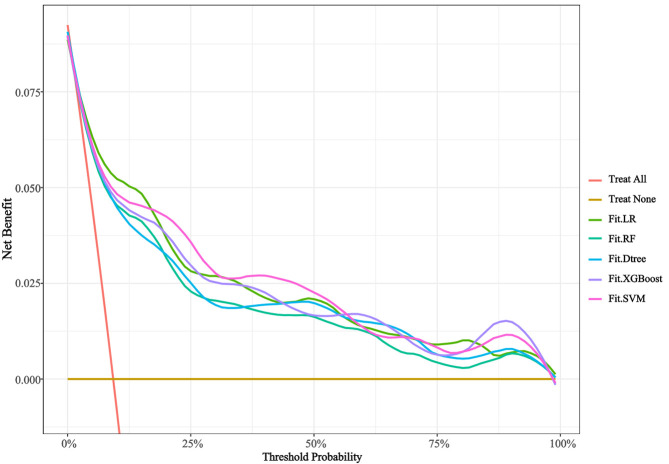
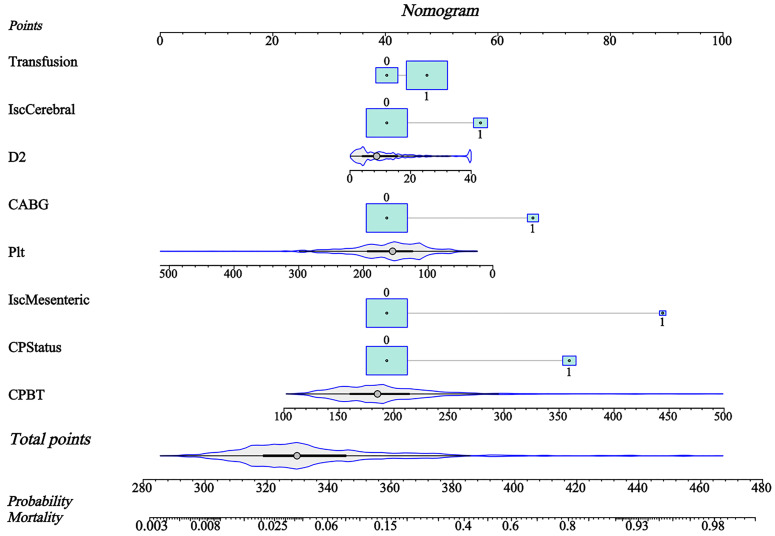
Results: The nomogram based on SVM outperformed others, achieving a mean area under the receiver operating characteristic (ROC) curve (AUC) of 0.842 on training dataset and a mean AUC of 0.782 on testing dataset, accompanied by a Brier score of 0.058. Key risk factors included cerebral malperfusion, mesenteric malperfusion, preoperative critical station, Marfan syndrome, platelet count, D-dimer, coronary artery bypass grafting, and cardiopulmonary bypass time. A web-based application was developed for clinical use.
Conclusions: We develop a novel nomogram risk prediction model based on SVM algorithm for in-hospital death following extended aortic arch repair for ATAAD with good discrimination and accuracy.
Clinical trial registration: Registration number ChiCTR2200066414, https://www.chictr.org.cn/showproj.html?proj=187074.
Keywords: acute type A aortic dissection; extended aortic arch repair; machine learning; nomogram; prediction model.
Copyright: © 2025 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Trimarchi S, Nienaber CA, Rampoldi V, Myrmel T, Suzuki T, Mehta RH, et al. Contemporary results of surgery in acute type A aortic dissection: The International Registry of Acute Aortic Dissection experience. The Journal of Thoracic and Cardiovascular Surgery . 2005;129:112–122. doi: 10.1016/j.jtcvs.2004.09.005. - DOI - PubMed
LinkOut - more resources
Full Text Sources
