

Hypocapnia and its relationship with in-hospital mortality in acute heart failure patients: Insights from the Indonesian multicenter ICCU registry
- PMID: 40352248
- PMCID: PMC12059876
- DOI: 10.52225/narra.v5i1.1638
Hypocapnia and its relationship with in-hospital mortality in acute heart failure patients: Insights from the Indonesian multicenter ICCU registry
Abstract
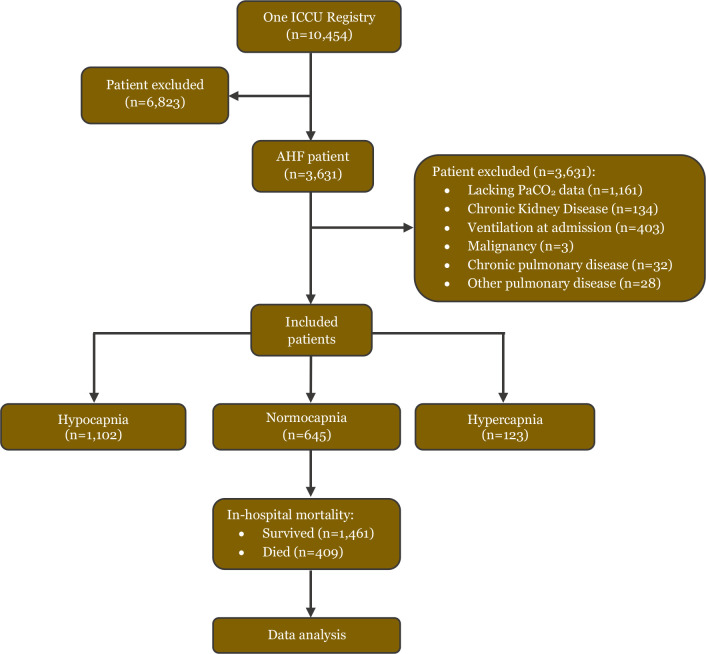
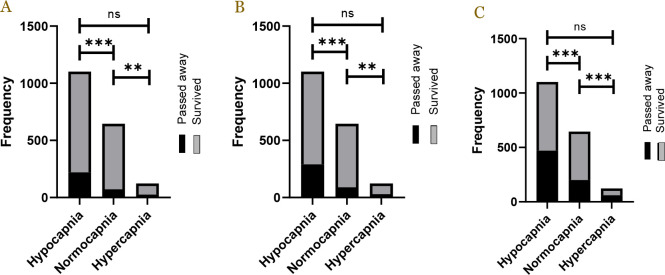
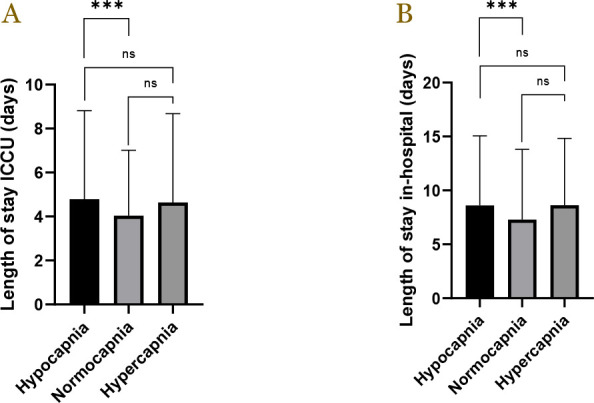
Acute heart failure (AHF) presents serious risks for hospitalized patients. The aim of this study was to explore the relationship between arterial partial pressure of carbon dioxide (PaCO2) levels and outcomes in AHF patients admitted to the intensive cardiovascular care unit (ICCU), utilizing data from the IndONEsia ICCU Registry (One ICCU Registry). A multicenter retrospective observational study was performed covering data between August 2021-2023. Participants were categorized by PaCO2 levels: hypocapnia (<35 mmHg), normocapnia (35-45 mmHg), and hypercapnia (>45 mmHg). The primary outcomes included ICCU mortality, in-hospital mortality, and 30-day mortality, whereas the length of the stays in the ICCU or hospital and ventilation requirement were set as the secondary outcomes. Mortality risks were assessed using Cox proportional hazards models. Of the 1,870 patients, 1,102 (58.96%) had hypocapnia, 645 (34.5%) had normocapnia, and 123 (6.5%) had hypercapnia. Hypocapnia patients had significantly higher ICCU, in-hospital, and at 30-day mortality rates compared to normocapnic patients (all p < 0.001), along with longer lengths of stay in ICCU and in hospital (p < 0.001). Hypocapnia significantly increased noninvasive and mechanical ventilation requirement compared to normocapnia patients. Multivariate analysis identified factors impacting patients' survival, including age, treatment with angiotensin-converting enzyme inhibitors (ACEi) / angiotensin II receptor blockers (ARBs) drugs, and severity scores such as the quick sequential organ failure assessment (qSOFA) and simplified acute physiology score II (SAPS II). In conclusion, hypocapnia in AHF patients could increase in-hospital, ICU and 30-days mortality rates and length of hospital stays, as well as noninvasive and mechanical ventilation requirements.
Keywords: Hypocapnia; ICCU; acute heart failure; in-hospital mortality; length of stay.
© 2025 The Author(s).
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical