

Clinical and molecular fingerprint of SARS-CoV-2 among hospital employees in a period of Omicron BA.2 dominance
- PMID: 40352653
- PMCID: PMC12059803
- DOI: 10.3205/dgkh000531
Clinical and molecular fingerprint of SARS-CoV-2 among hospital employees in a period of Omicron BA.2 dominance
Abstract
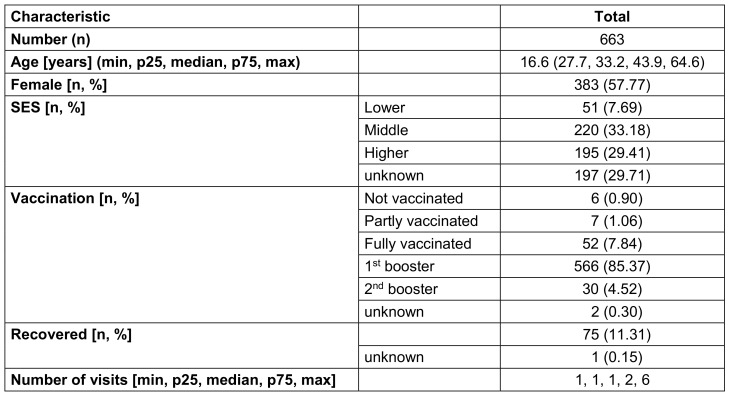
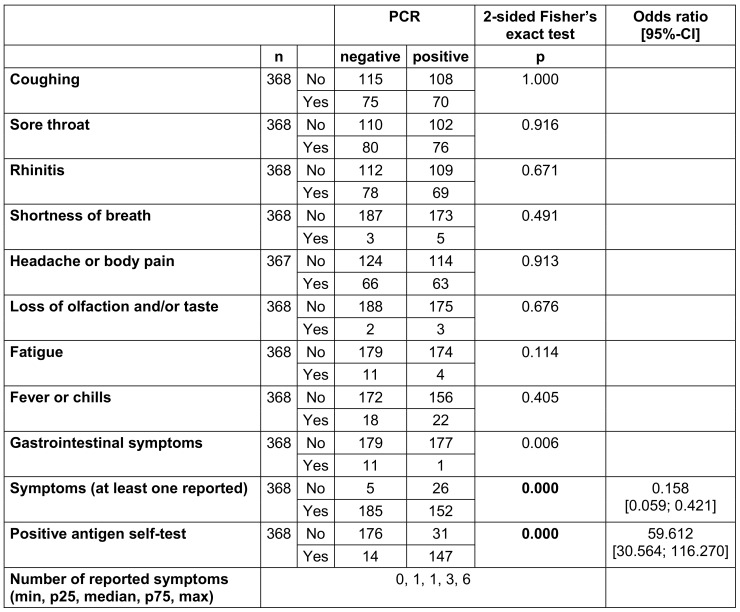
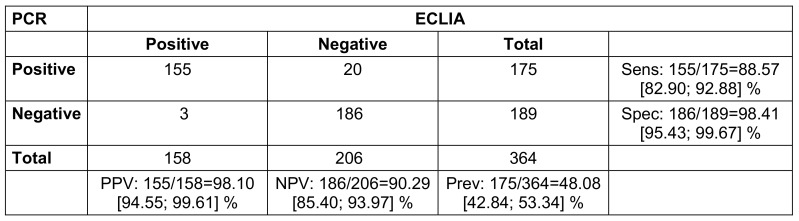
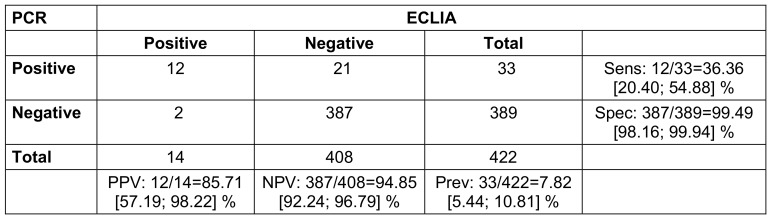
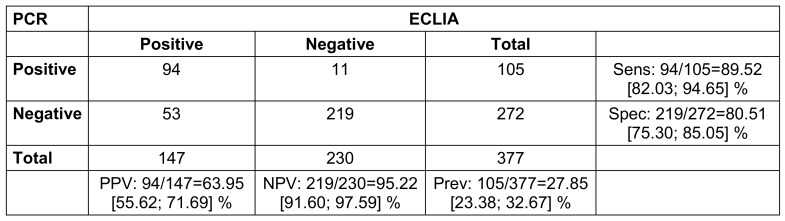
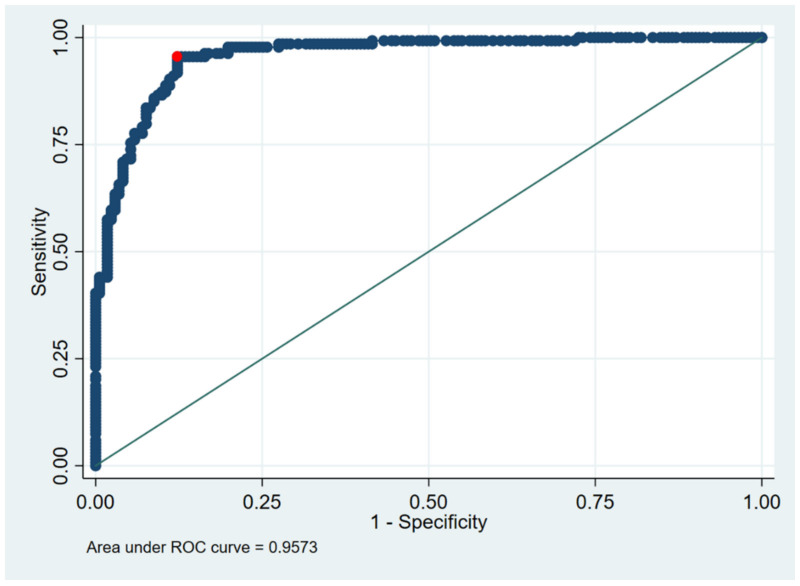
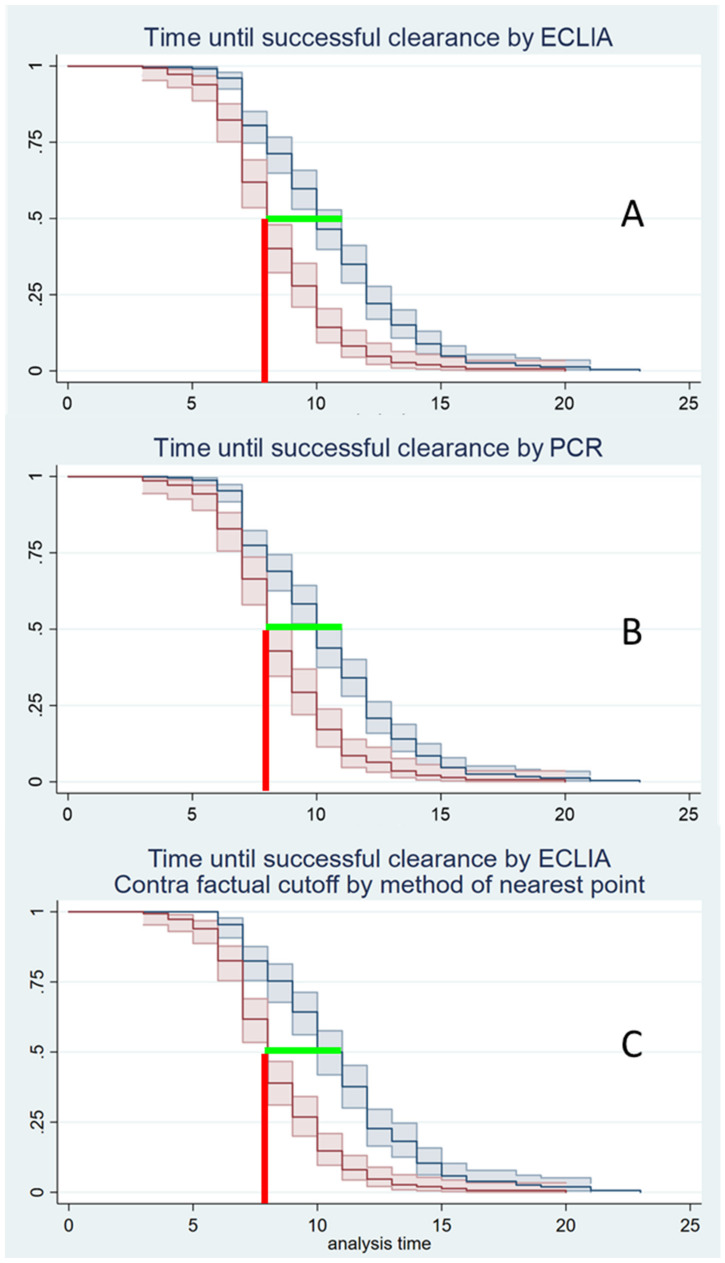
In the spring of 2022, SARS-CoV-2 Omicron BA.2 peaked in Germany. The main burden was staff shortage. To achieve effective identification and management of infected persons as well as early reintegration of recovered persons, an infection-control outpatient clinic was established at the Bundeswehr Central Hospital Koblenz. This article reports a secondary data analysis of 663 people with 1,174 visits to the outpatient clinic. For asymptomatic contacts, no correlation was observed between PCR result and testing time or frequency. Although no significant symptoms were documented, a high correlation was found between a positive antigen self-test and positive PCR. For clearance, a median time until a negative test was obtained was 8-11 days. The PCR gold standard was compared with ECLIA antigen testing for all indications. The results of this study challenge the rationale for testing asymptomatic contacts. Solely symptom-driven diagnostics by PCR also do not seem to be effective. However, contact persons or symptomatic persons with a positive rapid antigen test should be tested further. Whether this testing is done by ECLIA or PCR does not seem to matter. Clearance testing after recovery prior to day 8 is also not appropriate.
Im Frühjahr 2022 erreichte SARS-CoV-2 Omikron BA.2 in Deutschland seinen Höhepunkt. Die Hauptbelastung entstand durch Personalmangel. Um eine effektive Identifizierung und Behandlung von Infizierten sowie eine frühzeitige Wiedereingliederung von Erkrankten zu erreichen, wurde am Bundeswehrzentralkrankenhaus Koblenz eine Infektionsschutzambulanz eingerichtet. In diesem Artikel führen wir eine Sekundärdatenanalyse von 663 Personen mit 1.174 Besuchen in der Ambulanz durch. Bei asymptomatischen Kontakten konnte keine Korrelation zwischen PCR-Ergebnis und Testzeit oder -häufigkeit festgestellt werden. Wir konnten keine signifikanten Symptome feststellen, aber eine hohe Korrelation einem positiven Antigen-Selbsttest und einer positiven PCR. Für die Freitestung wurde eine mittlere Zeitspanne von 8–11 d bis zu einem negativen Test ermittelt. Wir haben den PCR-Goldstandard mit dem ECLIA-Antigentest für alle Indikationen verglichen. Unsere Ergebnisse stellen die Rationale für die Testung asymptomatischer Kontaktpersonen in Frage. Eine rein symptomorientierte Diagnostik mittels PCR scheint ebenfalls nicht effizient zu sein. Kontaktpersonen oder symptomatische Personen mit einem positiven Antigen-Schnelltest sollten jedoch weiter getestet werden. Ob diese Tests mittels ECLIA oder PCR durchgeführt werden, scheint keine Rolle zu spielen. Freitestung nach der Genesung vor dem 8. Tag sind ebenfalls nicht angebracht.
Keywords: COVID-19; COVID-19 symptoms; ECLIA; Omicron BA.2; SARS-CoV-2; antigen testing; clearance testing; contact testing; hospital hygiene; testing strategy.
Copyright © 2025 Rauschning et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
COVID-19 Symptoms and Duration of Rapid Antigen Test Positivity at a Community Testing and Surveillance Site During Pre-Delta, Delta, and Omicron BA.1 Periods.JAMA Netw Open. 2022 Oct 3;5(10):e2235844. doi: 10.1001/jamanetworkopen.2022.35844. JAMA Netw Open. 2022. PMID: 36215069 Free PMC article.
-
Clinical profile analysis of SARS-CoV-2 community infections during periods with omicron BA.2, BA.4/5, and XBB dominance in Hong Kong: a prospective cohort study.Lancet Infect Dis. 2025 Mar;25(3):276-289. doi: 10.1016/S1473-3099(24)00574-7. Epub 2024 Oct 14. Lancet Infect Dis. 2025. PMID: 39419049
-
SARS-CoV-2 rapid antigen test sensitivity and viral load in newly symptomatic hospital employees in Berlin, Germany, December, 2020 to February, 2022: an observational study.Lancet Microbe. 2024 Jun;5(6):e538-e546. doi: 10.1016/S2666-5247(23)00412-3. Epub 2024 May 14. Lancet Microbe. 2024. PMID: 38759669
-
Workplace interventions to reduce the risk of SARS-CoV-2 infection outside of healthcare settings.Cochrane Database Syst Rev. 2024 Apr 10;4(4):CD015112. doi: 10.1002/14651858.CD015112.pub3. Cochrane Database Syst Rev. 2024. PMID: 38597249 Free PMC article.
-
Universal screening for SARS-CoV-2 infection: a rapid review.Cochrane Database Syst Rev. 2020 Sep 15;9(9):CD013718. doi: 10.1002/14651858.CD013718. Cochrane Database Syst Rev. 2020. PMID: 33502003 Free PMC article.
References
-
- Dias VMCH, Oliveira AF, Marinho AKBB, Santos Ferreira CED, Domingues CEF, Fortaleza CMCB, Vidal CFL, Carrilho CMDM, Pinheiro DOBP, de Assis DB, Medeiros EA, Morejón KML, Weissmann L, Michelin L, Carneiro M, Nogueira MDSDP, de Oliveira PRD, Buralli RJ, Stucchi RSB, Lins RS, Costa SF, Chebabo A. COVID-19 and isolation: Risks and implications in the scenario of new variants. Braz J Infect Dis. 2022 Sep-Oct;26(5):102703. doi: 10.1016/j.bjid.2022.102703. - DOI - PMC - PubMed
-
- Baldi G, Berenberg-Gossler P, Engerer H, Junker S, Kholodilin KA, Kurcz F, Pagenhardt L. DIW Berlin economic outlook: Summer upswing to follow winter slump. DIW Wkly Rep. 2022;12(7/8):53–63. doi: 10.18723/diw_dwr:2022-7-1. - DOI
-
- Robert Koch-Institut. Wochenbericht vom 23.6.2022. 2022. [accessed 2022 Sep 18]. Available from: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsb....
-
- Neville S, Dombey D, Ghiglione D. Omicron sparks European health staff shortages but spares ICUs. Feb 06, 2022. [accessed 2024 Oct 18]. Available from: https://www.ft.com/content/dfea2eee-cc89-44bd-bad0-de04741cd179.
-
- Cremades-Martínez P, Parker LA, Chilet-Rosell E, Lumbreras B. Evaluation of Diagnostic Strategies for Identifying SARS-CoV-2 Infection in Clinical Practice: a Systematic Review and Compliance with the Standards for Reporting Diagnostic Accuracy Studies Guideline (STARD) Microbiol Spectr. 2022 Aug 31;10(4):e0030022. doi: 10.1128/spectrum.00300-22. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
