

Fulminant simultaneous multiple dissections of the cervical and vertebral arteries leading to hemorrhagic and ischemic stroke: A case report
- PMID: 40353159
- PMCID: PMC12065484
- DOI: 10.25259/SNI_167_2025
Fulminant simultaneous multiple dissections of the cervical and vertebral arteries leading to hemorrhagic and ischemic stroke: A case report
Abstract
Background: Intra-and extracranial artery dissections are uncommon but significant causes of ischemic stroke and subarachnoid hemorrhage (SAH). While individual dissections are well-documented, simultaneous dissections of multiple vessels leading to both hemorrhagic and ischemic strokes are extremely rare.
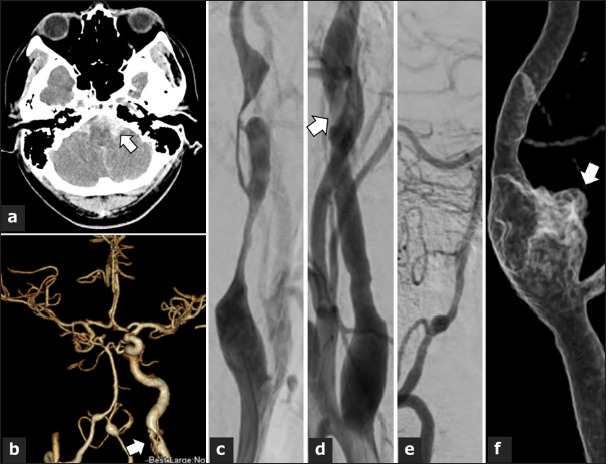
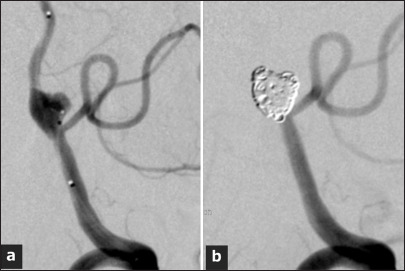
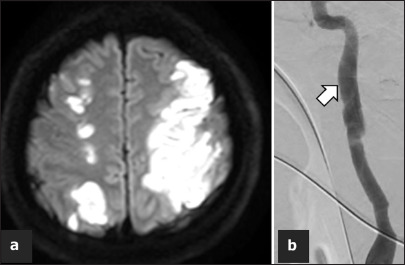
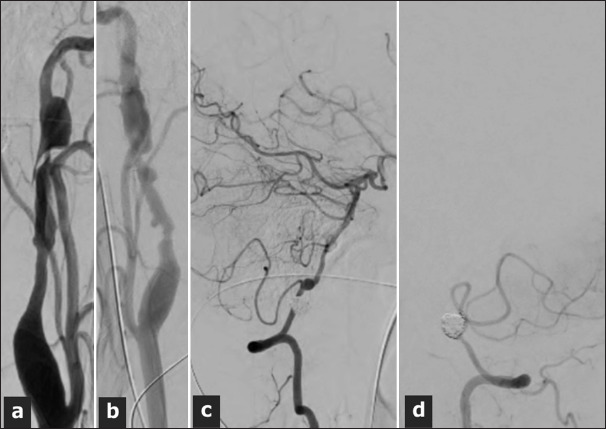
Case description: A 41-year-old man presented with acute onset of headache, vomiting, and loss of consciousness. Imaging revealed multiple arterial dissections involving the bilateral internal carotid arteries and vertebral arteries (VAs). The patient was diagnosed with SAH caused by a ruptured fusiform aneurysm in the left VA. Emergency endovascular trapping was performed to treat the ruptured VA aneurysm. The following day, ischemic infarctions were observed in both hemispheres, prompting the initiation of dual antiplatelet therapy for the cervical carotid artery dissection. Despite the complexity of his condition, the patient achieved functional recovery, with a modified Rankin Scale score of 3 at discharge.
Conclusion: Simultaneous hemorrhagic and ischemic strokes due to multiple arterial dissections pose significant diagnostic and therapeutic challenges. This case highlights the importance of individualized treatment strategies and calls for further research to establish evidence-based guidelines for managing such complex conditions.
Keywords: Cerebral infarction; Internal trapping; Multiple dissection; Subarachnoid hemorrhage.
Copyright: © 2025 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Béjot Y, Aboa-Eboulé C, Debette S, Pezzini A, Tatlisumak T, Engelter S, et al. Characteristics and outcomes of patients with multiple cervical artery dissection. Stroke. 2014;45:37–41. - PubMed
-
- Bond KM, Krings T, Lanzino G, Brinjikji W. Intracranial dissections: A pictorial review of pathophysiology, imaging features, and natural history. J Neuroradiol. 2021;48:176–88. - PubMed
-
- Brkić BG, Jaramaz TD, Vukičević M, Stanisavljević N, Kostić D, Lučić M, et al. Vertebrobasilar and internal carotid arteries dissection in 188 patients. J Clin Neurosci. 2021;93:6–16. - PubMed
-
- Debette S, Compter A, Labeyrie MA, Uyttenboogaart M, Metso TM, Majersik JJ, et al. Epidemiology, pathophysiology, diagnosis, and management of intracranial artery dissection. Lancet Neurol. 2015;14:640–54. - PubMed
-
- Hassan AE, Zacharatos H, Mohammad YM, Tariq N, Vazquez G, Rodriguez GJ, et al. Comparison of single versus multiple spontaneous extra-and/or intracranial arterial dissection. J Stroke Cerebrovasc Dis. 2013;22:42–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources