

The efficacy of neurostimulation techniques for the management of chronic pain associated with bone disorders: A systematic review and meta-analysis
- PMID: 40353170
- PMCID: PMC12065503
- DOI: 10.25259/SNI_521_2024
The efficacy of neurostimulation techniques for the management of chronic pain associated with bone disorders: A systematic review and meta-analysis
Abstract
Background: The management of chronic pain associated with bone problems has been accomplished by the use of neurostimulation methods, such as spinal cord stimulation (SCS) and peripheral nerve stimulation (PNS). It is still unknown, however, how successful they are in comparison. The effectiveness of SCS and PNS in reducing chronic pain and enhancing functional results in patients with chronic pain related to bone abnormalities was assessed in this comprehensive review and meta-analysis.
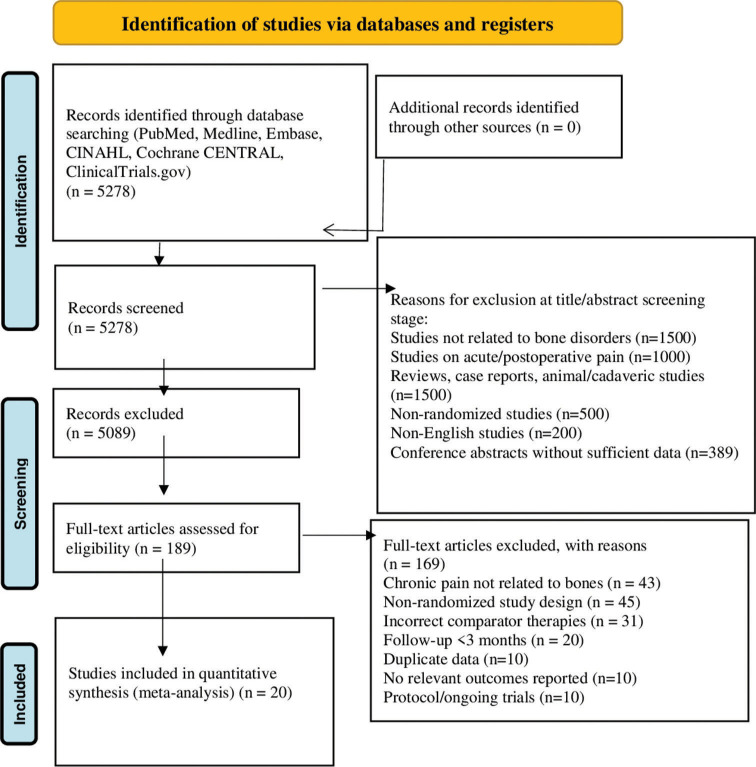
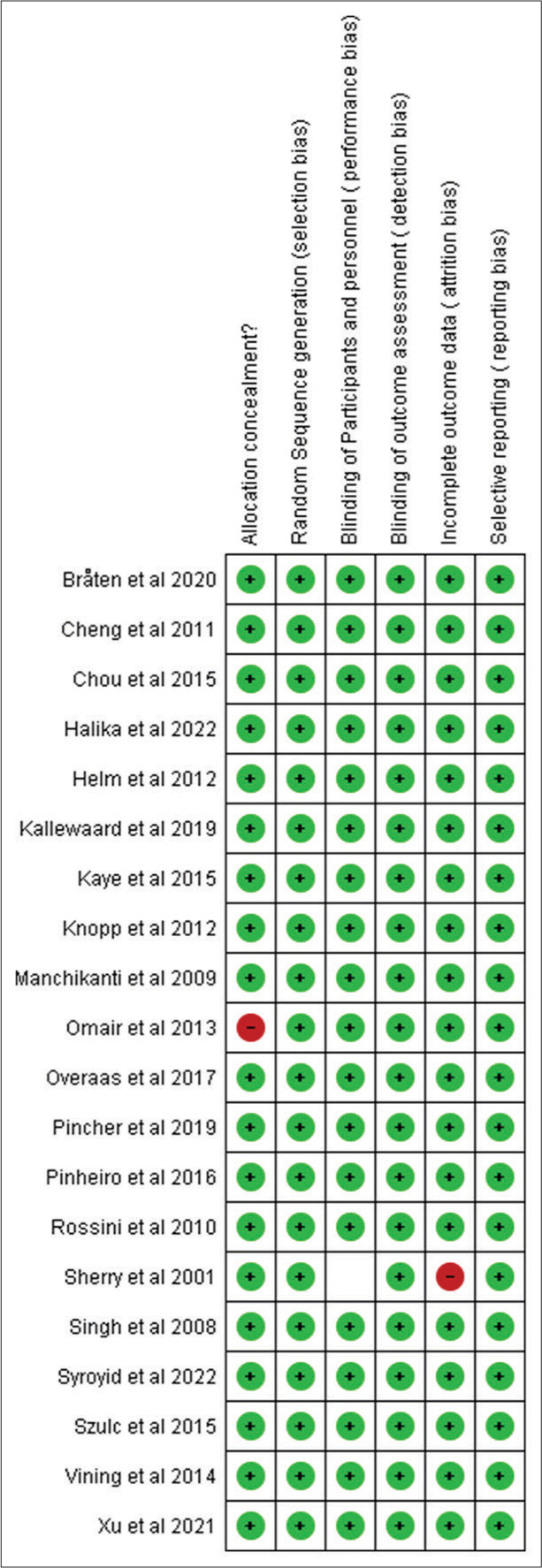
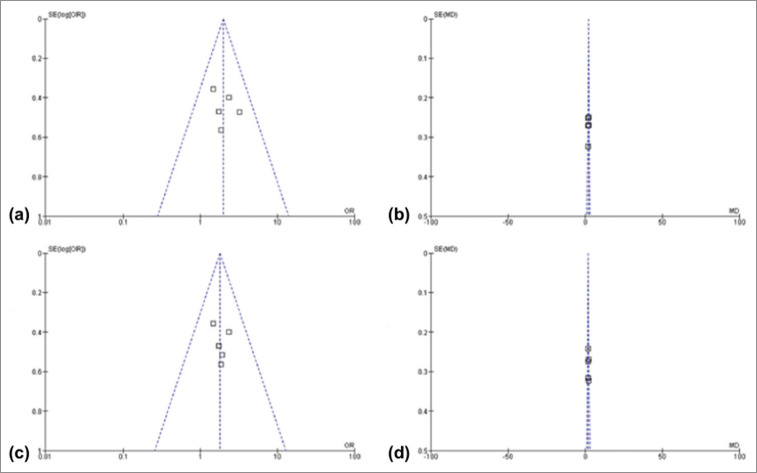
Methods: To find randomized controlled trials (RCTs) comparing SCS or PNS to standard medical management or placebo/sham treatment in adults with chronic pain related to bone disorders, a comprehensive search of PubMed, MEDLINE, Embase, CINAHL, Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov was carried out from the start of the database until February 2024. The main result was the absence of discomfort. Opioid usage, functional status, and quality of life were secondary outcomes. The Cochrane technique was used to evaluate bias risk. The risk ratios (RRs) or standardized mean differences (SMDs) with 95% confidence intervals (CIs) were computed using random effects meta-analysis.
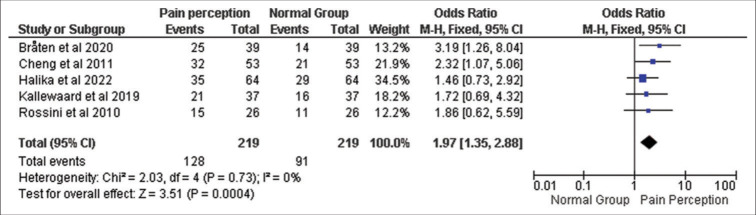
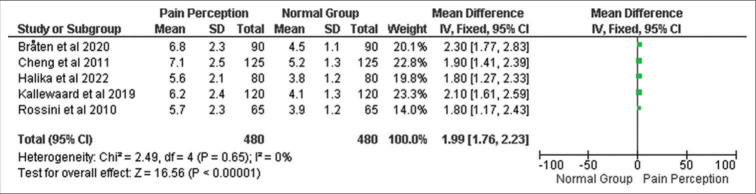
Results: We included 20 RCTs with a total of 2576 participants. In short-term (≤6 months) follow-up, SCS and PNS were both associated with substantially higher pain alleviation than conventional medical care or placebo/sham: SCS SMD -0.87 (95% CI -1.19--0.55), PNS SMD -0.56 (95% CI -0.91-0.21). SCS SMD -0.71 (95% CI -1.05--0.37) and PNS SMD -0.60 (95% CI -1.03--0.17) benefits were maintained at long-term (>6 months) follow-up. The physical and emotional functioning, as well as quality of life, were also markedly enhanced by SCS and PNS. It was shown that SCS (RR 0.57, 95% CI 0.44-0.74) and PNS (RR 0.58, 95% CI 0.43-0.77) reduced the risk of opioid usage.
Conclusion: When it comes to improving functionality and quality of life, SCS and PNS both reduce chronic pain linked to bone problems, both temporarily and permanently. In some individuals, SCS and PNS may assist in lowering opioid consumption. Neurostimulation treatments may be useful in the treatment of persistent pain associated with bone diseases.
Keywords: Bone disorders; Chronic pain; Meta-analysis; Peripheral nerve stimulation; Spinal cord stimulation; Systematic review.
Copyright: © 2025 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures



References
-
- Bobos P, Pereira TV, Pouliopoulou DV, Charakopoulou-Travlou M, Nazari G, MacDermid JC. Which remote rehabilitation interventions work best for chronic musculoskeletal pain and depression? A Bayesian network meta-analysis. J Orthop Sports Phys Ther. 2024;54:361–76. - PubMed
-
- Bråten LC, Schistad EI, Espeland A, Kristoffersen PM, Haugen AJ, Marchand GH, et al. Association of modic change types and their short tau inversion recovery signals with clinical characteristics: A cross-sectional study of chronic low back pain patients in the AIM-study. BMC Musculoskelet Disord. 2020;21:368. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources