

[Dynamic changes in genetic mutations in myelodysplastic neoplasms with progressive disease and leukemic transformation]
- PMID: 40355355
- PMCID: PMC12038471
- DOI: 10.3760/cma.j.cn121090-20240708-00254
[Dynamic changes in genetic mutations in myelodysplastic neoplasms with progressive disease and leukemic transformation]
Abstract
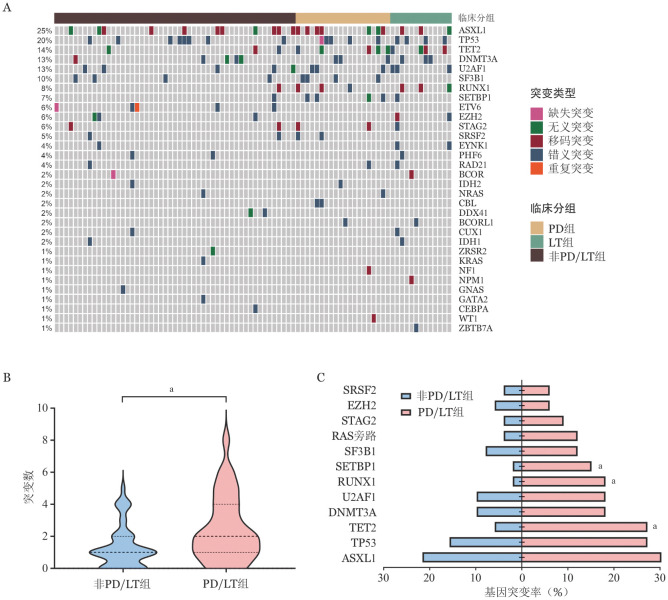
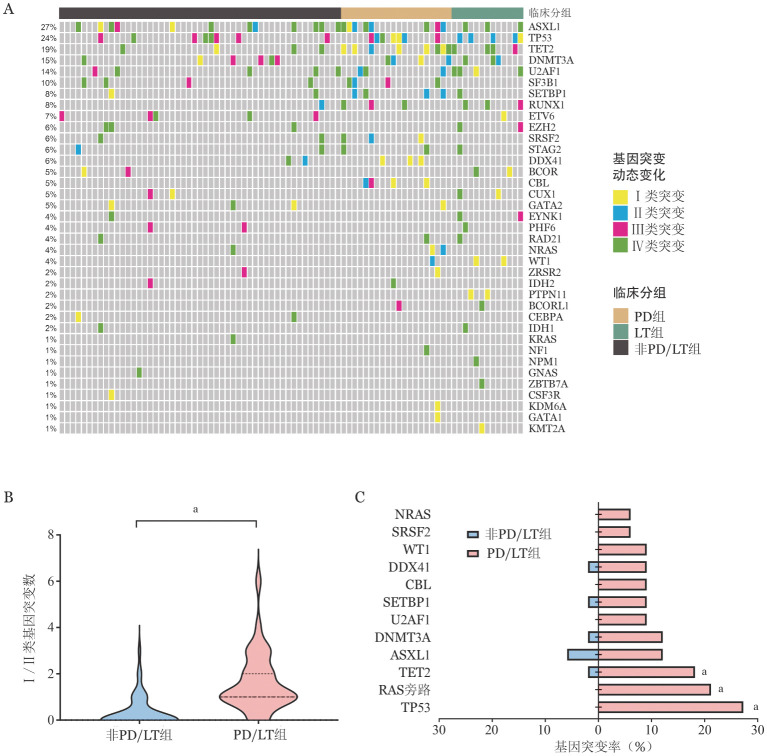
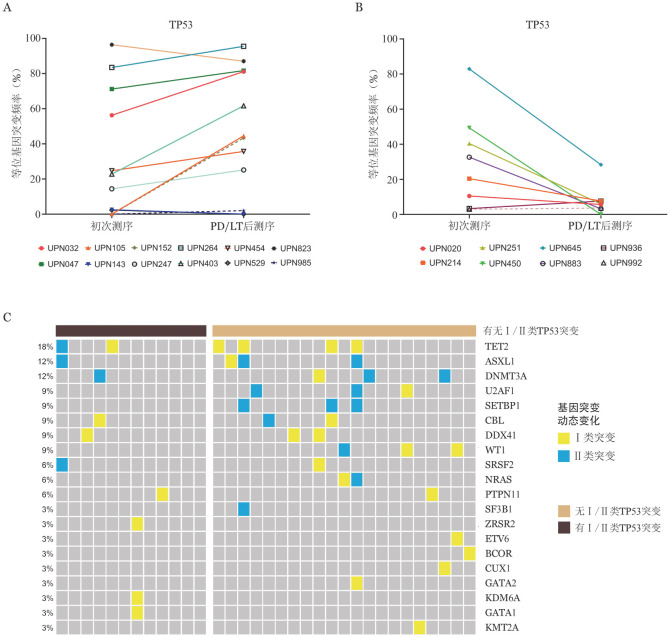
Objective: To investigate the key genetic mutations during the progressive disease (PD) /leukemic transformation (LT) course in MDS by analyzing the dynamic changes of genetic mutations in patients with myelodysplastic neoplasms (MDS) with or without PD/LT. Methods: This study enrolled 84 patients with sequential MDS from May 2019 to August 2023 at ZhongDa Hospital Southeast University and used the next generation sequencing to detect gene mutations. The dynamic changes of genetic mutations in patients with MDS with or without PD/LT were retrospectively analyzed. Results: ①This study analyzed data from 84 patients diagnosed with MDS with a median age of 63 (range: 31-95) years and consisting of 51 males and 33 females. Participants were distributed to the PD cohort (n=20), LT cohort (n=13), and non-PD/LT cohort (n=51). Patients from the PD/LT cohorts demonstrated a higher proportion of bone marrow blasts than the non-PD/LT cohort at the first sequencing (1.6% vs. 0.4%, P=0.013). ②The most frequently mutated genes that were detected at first sequencing were ASXL1 (n=21, 25.0%), TP53 (n=17, 20.2%), TET2 (n=12, 14.3%), DNMT3A (n=11, 13.1%), and U2AF1 (n=11, 13.1%). Further, patients from the PD/LT cohorts exhibited a higher median number of mutated genes than the non-PD/LT cohort (2 vs.1, P=0.014) at first sequencing. TET2 (27.3% vs. 5.9%, P=0.010), SETBP1 (15.2% vs.2.0%, P=0.033), and RUNX1 (18.2% vs. 2.0%, P=0.013) mutations were enriched in the PD/LT cohorts than in the non-PD/LT cohort. ③The most frequently detected acquired mutations (Ⅰ mutations) and clonally expanded mutations (Ⅱ mutations) were TP53 (n=9, 10.7%), TET2 (n=7, 8.3%), ASXL1 (n=7, 8.3%), and RAS pathway (n=7, 8.3%). Furthermore, patients from the PD/LT cohorts showed a higher median number of Ⅰ/Ⅱ genes than the non-PD/LT cohort (2 vs. 0, P<0.001), and Ⅰ/Ⅱ RAS pathway (21.2% vs. 0, P=0.001), TP53 (27.3% vs. 0, P<0.001), and TET2 (18.2% vs. 2.0%, P=0.013) mutations were enriched in PD/LT cohorts than in the non-PD/LT cohorts. ④Most of the TP53 mutations (9/12, 75.0%) in PD/LT cohorts were Ⅰ/Ⅱ mutations, whereas all of the TP53 mutations in non-PD/LT cohort were clone-decrease mutations (Ⅲ mutations) (5/8, 62.5%) or clone-stable mutations (Ⅳ mutations) (3/8, 37.5%). Most of the RAS pathway mutations (7/8,87.5%) in the PD/LT cohorts were Ⅰ/Ⅱ mutations, whereas only one patient in the non-PD/LT cohort demonstrated RAS pathway mutations, which belonged to Ⅳ mutations. Conclusion: Patients from the PD/LT cohorts demonstrated a higher proportion of bone marrow blasts and a higher median number of mutations than the non-PD/LT cohort at first sequencing; TET2, SETBP1, and RUNX1 mutations were enriched in the PD/LT cohorts than in the non-PD/LT cohort at first sequencing. Patients from the PD/LT cohorts exhibited a higher number of Ⅰ/Ⅱ mutations than the non-PD/LT cohort. Further, Ⅰ/Ⅱ TP53, RAS pathway, and TET2 mutations were enriched in the PD/LT cohorts, and Ⅰ/Ⅱ TP53 and RAS pathway mutations may contribute to the PD/LT.
目的: 分析骨髓增生异常肿瘤(Myelodysplastic neoplasms, MDS)疾病进展(Progressive disease, PD)/白血病转化(Leukemic transformattion, LT)组和非PD/LT组患者病程中基因突变动态变化差异,探索在MDS发生PD/LT过程中起关键作用的基因突变。 方法: 收集2019年5月至2023年8月于东南大学附属中大医院就诊的至少有2次高通量二代测序(Next generation sequencing, NGS)基因突变结果的84例MDS患者,比较PD/LT组和非PD/LT组患者病程中基因突变动态变化差异。 结果: ①84例患者中男性51例,女性33例,初次测序时中位年龄69(31~95)岁。PD组20例,LT组13例,非PD/LT组51例。初次测序时PD/LT组中位骨髓原始细胞比例高于非PD/LT组(1.6%对0.4%,P=0.013)。②84例患者初次测序时基因突变检出率较高的依次为ASXL1(21例,25.0%)、TP53(17例,20.2%)、TET2(12例,14.3%)、DNMT3A(11例,13.1%)、U2AF1(11例,13.1%);PD/LT组患者初次测序时中位基因突变个数高于非PD/LT组(2个对1个,P=0.014);PD/LT组初次测序时TET2(27.3%对5.9%,P=0.010)、SETBP1(15.2%对2.0%,P=0.033)、RUNX1(18.2%对2.0%,P=0.013)突变比例高于非PD/LT组。③84例患者病程中检出率较高的新增突变(Ⅰ类突变)/克隆扩增突变(Ⅱ类突变)依次为TP53(9例,10.7%)、TET2(7例,8.3%)、ASXL1(7例,8.3%)、RAS旁路突变(7例,8.3%);PD/LT组中位Ⅰ/Ⅱ类基因突变数目显著高于非PD/LT组(2个对0个,P<0.001)。PD/LT组患者Ⅰ/Ⅱ类RAS旁路(21.2%对0,P=0.001)、TP53(27.3%对0,P<0.001)、TET2(18.2%对2.0%,P=0.013)突变比例显著高于非PD/LT组。④PD/LT组75.0%(9/12)患者TP53突变为Ⅰ/Ⅱ类突变;非PD/LT组患者TP53突变皆为克隆缩小(Ⅲ类突变)(5/8,62.5%)或克隆稳定突变(Ⅳ类突变)(3/8,37.5%)。PD/LT组87.5%(7/8)的患者RAS旁路突变为Ⅰ/Ⅱ类突变;非PD/LT组患者仅有1例病程中有RAS旁路突变,为Ⅳ类突变。 结论: PD/LT组患者初次测序时中位骨髓原始细胞比例和基因突变数目高于非PD/LT组;TET2、SETBP1、RUNX1突变比例高于非PD/LT组。PD/LT组中位Ⅰ/Ⅱ类基因突变数目和Ⅰ/Ⅱ类TP53、RAS旁路、TET2基因突变比例高于非PD/LT组。Ⅰ/Ⅱ类TP53和RAS旁路突变可能在MDS发生PD/LT过程中起关键作用。.
Keywords: Dynamic changes; Leukemic transformation; Myelodysplastic neoplasms; Progressive disease.
Conflict of interest statement
Figures
Similar articles
-
[Analysis of Gene Mutation and Clinical Characteristics Related to Myelodysplastic Syndrome].Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2024 Dec;32(6):1798-1806. doi: 10.19746/j.cnki.issn.1009-2137.2024.06.025. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2024. PMID: 39743268 Chinese.
-
Prognostic impact of DTA mutation and co-occurring mutations in patients with myelodysplastic syndrome.Mol Biol Rep. 2024 Sep 15;51(1):985. doi: 10.1007/s11033-024-09922-7. Mol Biol Rep. 2024. PMID: 39278886
-
Impact of the variant allele frequency of ASXL1, DNMT3A, JAK2, TET2, TP53, and NPM1 on the outcomes of patients with newly diagnosed acute myeloid leukemia.Cancer. 2020 Feb 15;126(4):765-774. doi: 10.1002/cncr.32566. Epub 2019 Nov 19. Cancer. 2020. PMID: 31742675
-
[Research progress on genes associated with transformation of myelodysplastic syndromes to acute myeloid leukemia].Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2014 Jun;22(3):873-8. doi: 10.7534/j.issn.1009-2137.2014.03.057. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2014. PMID: 24989313 Review. Chinese.
-
Routine clinical mutation profiling using next generation sequencing and a customized gene panel improves diagnostic precision in myeloid neoplasms.Oncotarget. 2016 May 24;7(21):30084-93. doi: 10.18632/oncotarget.8310. Oncotarget. 2016. PMID: 27029036 Free PMC article. Review.
References
-
- 中华医学会血液学分会. 骨髓增生异常综合征中国诊断与治疗指南(2019年版)[J] 中华血液学杂志. 2019;40(2):89–97. doi: 10.3760/cma.j.issn.0253-2727.2019.02.001. - DOI
- Chinese Society of Hematology, Chinese Medical Association. Chinese guidelines for diagnosis and treatment of myelodysplastic syndromes (2019)[J] Chin J Hematol. 2019;40(2):89–97. doi: 10.3760/cma.j.issn.0253-2727.2019.02.001. - DOI - PMC - PubMed
-
- 赵 颂扬, 徐 泽锋, 秦 铁军, et al. 骨髓增生异常综合征白血病转化危险因素研究[J] 中华血液学杂志. 2022;43(10):818–825. doi: 10.3760/cma.j.issn.0253-2727.2022.10.004. - DOI
- Zhao SY, Xu ZF, Qin TJ, et al. Risk factors for leukemia transformation in patients with myelodysplastic syndromes[J] Chin J Hematol. 2022;43(10):818–825. doi: 10.3760/cma.j.issn.0253-2727.2022.10.004. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous