

Establishing a Prediction Model for Weight Loss Outcomes After LSG in Chinese Obese Patients with BMI ≥ 32.5 Kg/m2 Using Body Composition Data
- PMID: 40356711
- PMCID: PMC12067650
- DOI: 10.2147/DMSO.S508067
Establishing a Prediction Model for Weight Loss Outcomes After LSG in Chinese Obese Patients with BMI ≥ 32.5 Kg/m2 Using Body Composition Data
Abstract
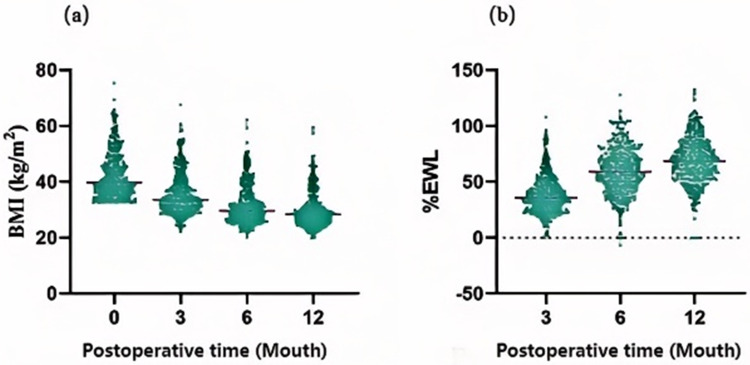
Background: Laparoscopic sleeve gastrectomy (LSG) is associated with sustained and substantial weight loss. However, suboptimal results are observed in certain patients.
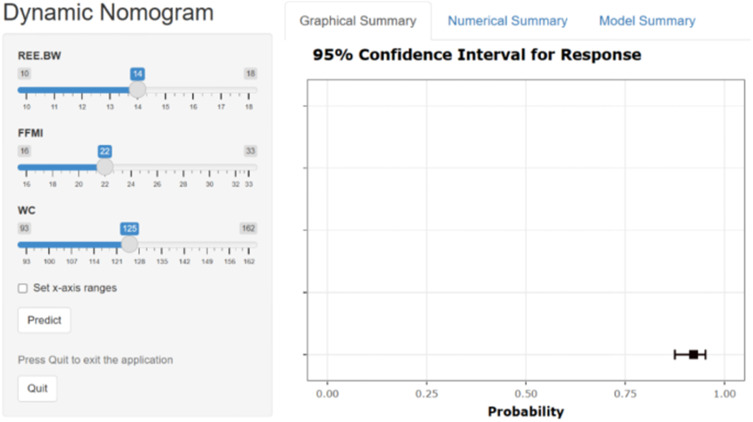
Objective: Drawing from body composition data at our center, clinically accessible predictive factors for weight loss outcomes were identified, leading to the development and validation of a preoperative predictive model for weight loss following LSG.
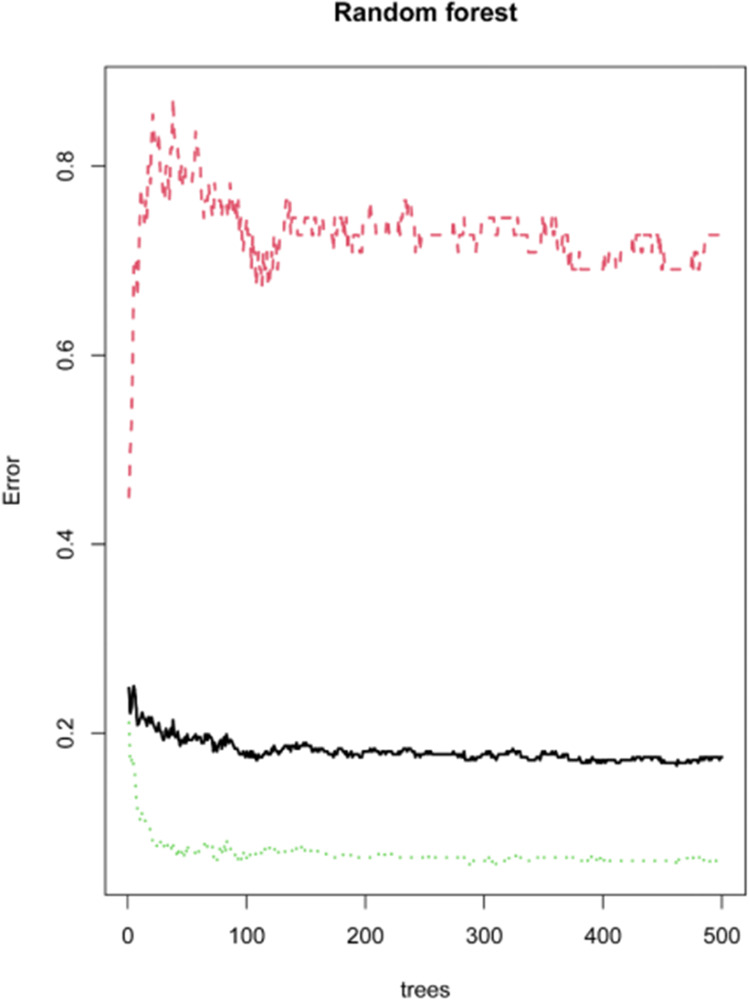
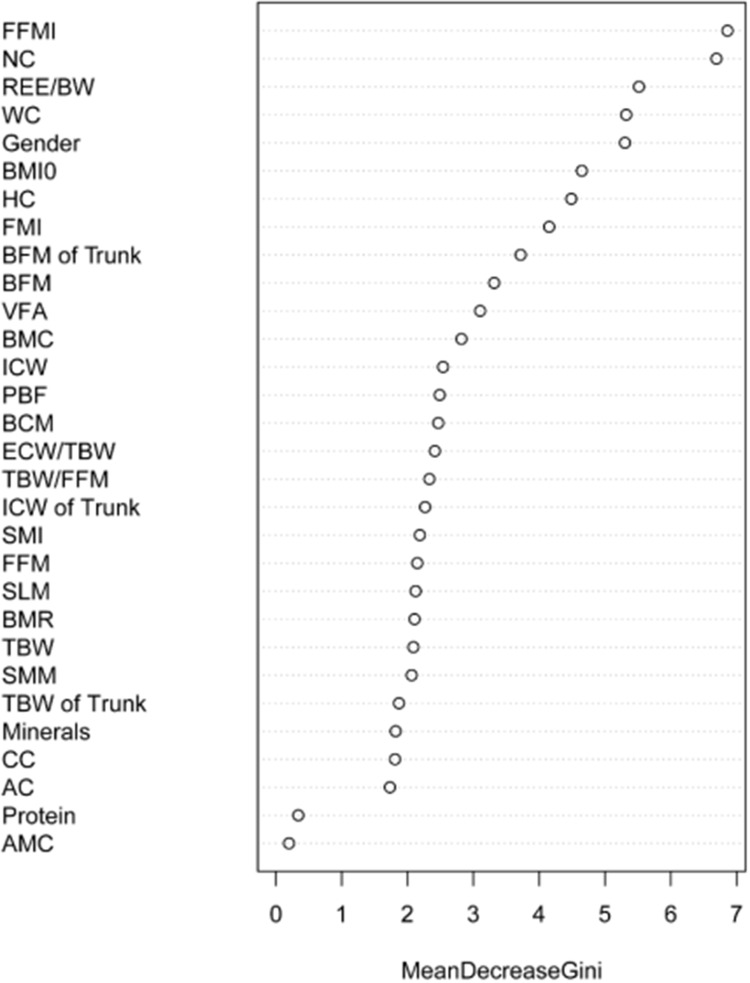
Methods and materials: A retrospective analysis was conducted on the general clinical baseline and body composition data of obese patients (body mass index [BMI] ≥ 32.5 kg/m2) who underwent LSG between December 2016 and December 2022. Independent predictors for weight loss outcomes were selected through univariate logistic regression, random forest analysis, and multivariate logistic regression. Subsequently, a nomogram was developed to predict weight loss outcomes and was evaluated for discrimination, accuracy, and clinical utility, with validation performed in a separate cohort.
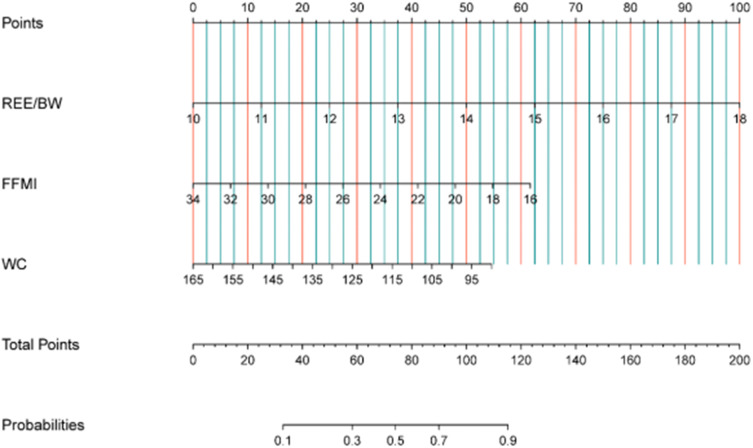
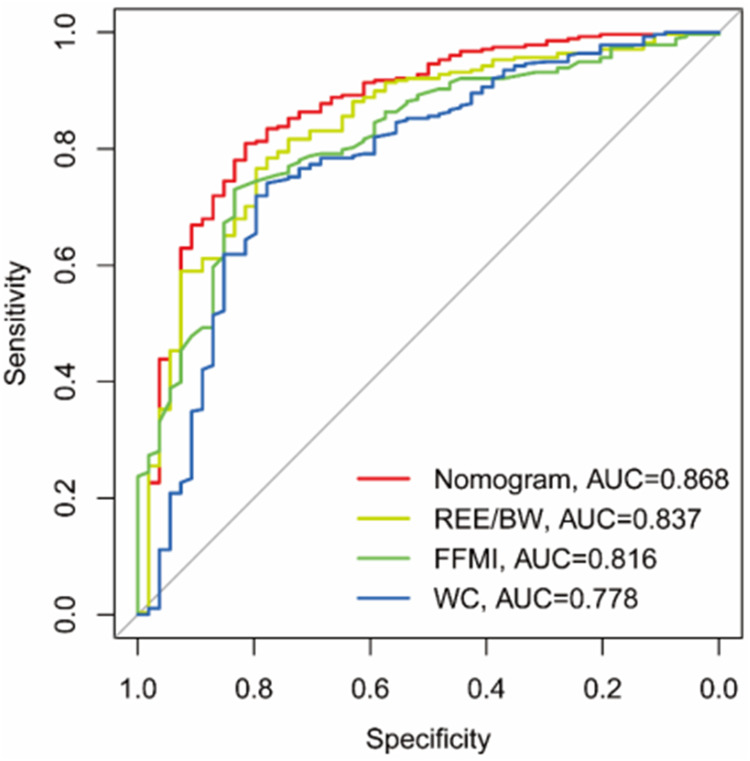
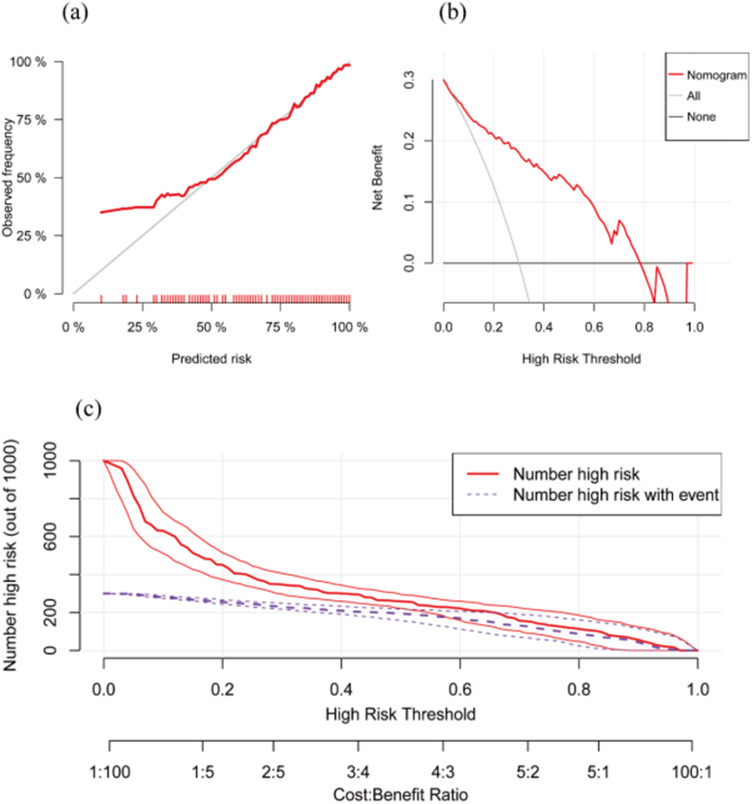
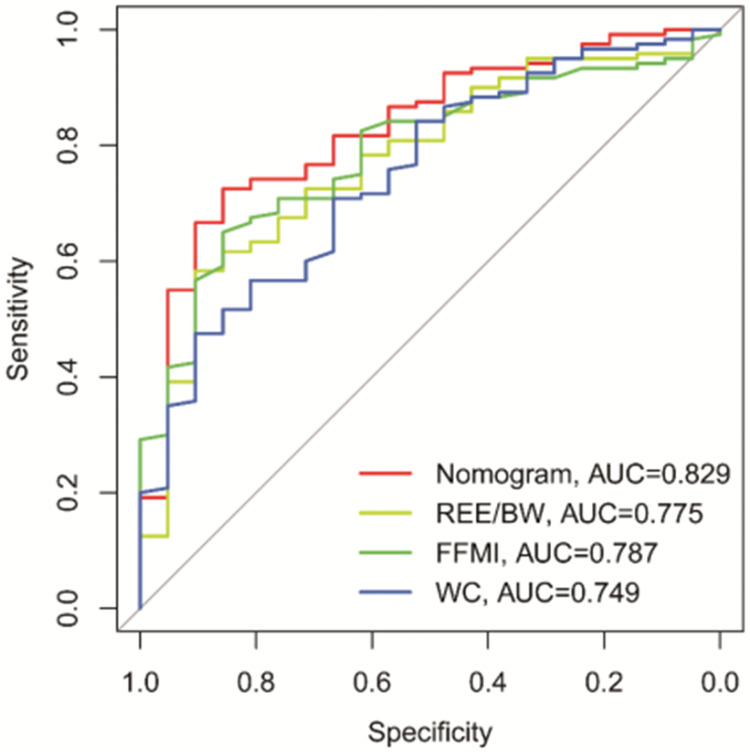
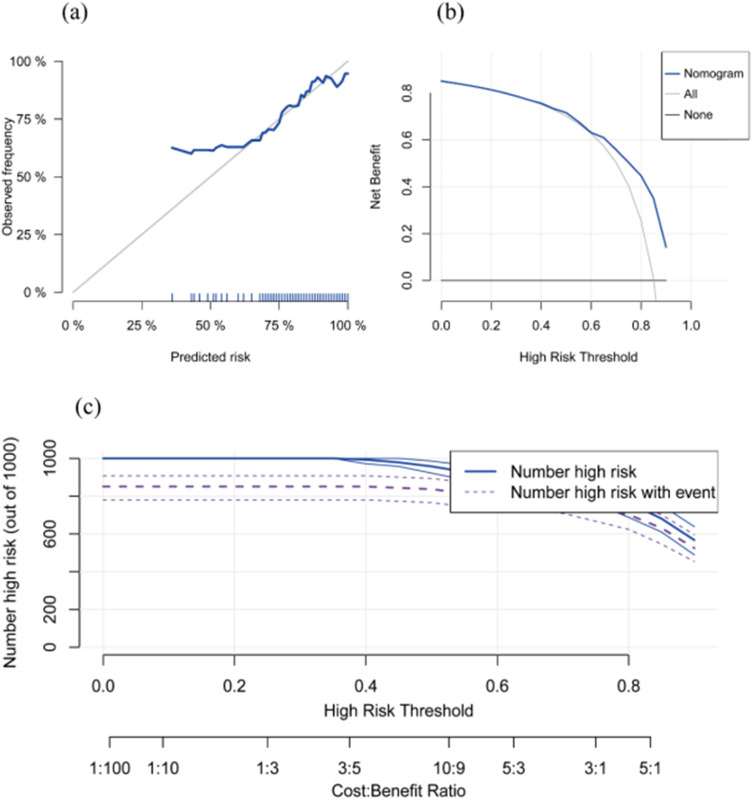
Results: A total of 473 patients with mean BMI were included. The preoperative resting energy expenditure to body weight ratio (REE/BW), fat-free mass index (FFMI), and waist circumference (WC) emerged as independent predictive factors for weight loss outcomes at one year post-LSG. These body composition parameters were incorporated into the construction of an Inbody predictive nomogram, which yielded area under the curve (AUC) values of 0.868 (95% CI: 0.826-0.902) for the modeling cohort and 0.829 (95% CI: 0.756-0.887) for the validation cohort. Calibration curves, decision curve analysis (DCA), and clinical impact curves (CIC) from both groups demonstrated the model's robust discrimination, accuracy, and clinical utility.
Conclusion: In obese Chinese patients with a BMI ≥ 32.5 kg/m2, the Inbody-based nomogram integrating REE/BW, FFMI, and WC offers an effective preoperative tool for predicting weight loss outcomes one year after LSG, facilitating surgical planning and postoperative management.
Keywords: body composition data; laparoscopic sleeve gastrectomy; metabolic bariatric surgery; obesity; prognostic prediction.
© 2025 Wang et al.
Conflict of interest statement
Liang Wang, Yilan Sun and Qing Sang are co-first authors for this study. The authors report no conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
