

Sex differences in the sensitization of prenatally programmed hypertension
- PMID: 40356772
- PMCID: PMC12066558
- DOI: 10.3389/fphys.2025.1589615
Sex differences in the sensitization of prenatally programmed hypertension
Abstract
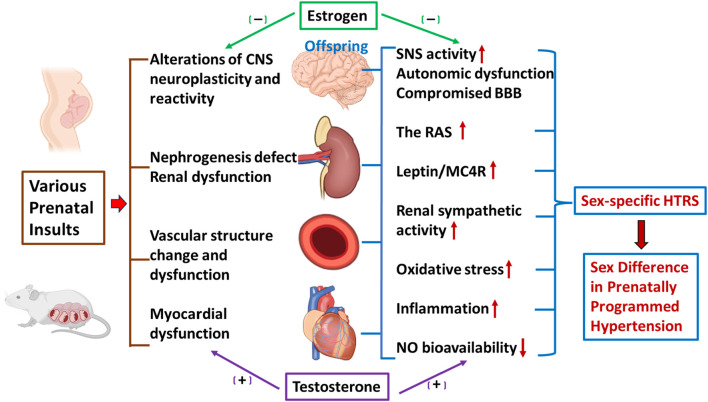
Studies have demonstrated that there are sex differences in the timing of onset and severity of prenatally programmed hypertension, with consistently milder phenotypes observed in females relative to male offspring. However, the root cause(s) for these sex-specific effects is unknown. Activation of the renin-angiotensin system (RAS), elevated oxidative stress and inflammation, and sympathetic hyperactivity in the cardiovascular organs and cardiovascular regulatory systems, are all involved in the pathogenesis of hypertension. Sex hormones interact with these prohypertensive systems to modulate blood pressure, and this interaction may lead to a sex-specific development of programmed hypertension. A more complete understanding of the functional capabilities of the sex hormones and their interactions with prohypertensive factors in offspring, from early life to aging, would likely lead to new insights into the basis of sex differences in programmed hypertension. Recently, we have discovered that sex differences also occur in the sensitization of offspring hypertension as programmed by maternal gestational hypertension and that this requires the brain RAS and proinflammatory factors. In this review, we will discuss the possible mechanisms underlying sex differences in sensitization to hypertension in the offspring of mothers exposed to various prenatal insults. These mechanisms operate at various levels from the periphery to the central nervous system (e.g., blood vessel, heart, kidney, and brain). Understanding the sex-specific mechanisms responsible for the sensitized state in offspring can help to develop therapeutic strategies for interrupting the vicious cycle of transgenerational hypertension and for treating hypertension in men and women differentially to maximize efficacy.
Keywords: blood pressure; inflammation; prenatal programming; renin-angiotensin system; sensitization; sex differences.
Copyright © 2025 Xue, Johnson and Bassuk.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources