

Augmented reality visualization of biomechanical wall stresses on abdominal aortic aneurysms using artificial intelligence
- PMID: 40357002
- PMCID: PMC12068883
- DOI: 10.1016/j.sctalk.2025.100432
Augmented reality visualization of biomechanical wall stresses on abdominal aortic aneurysms using artificial intelligence
Abstract
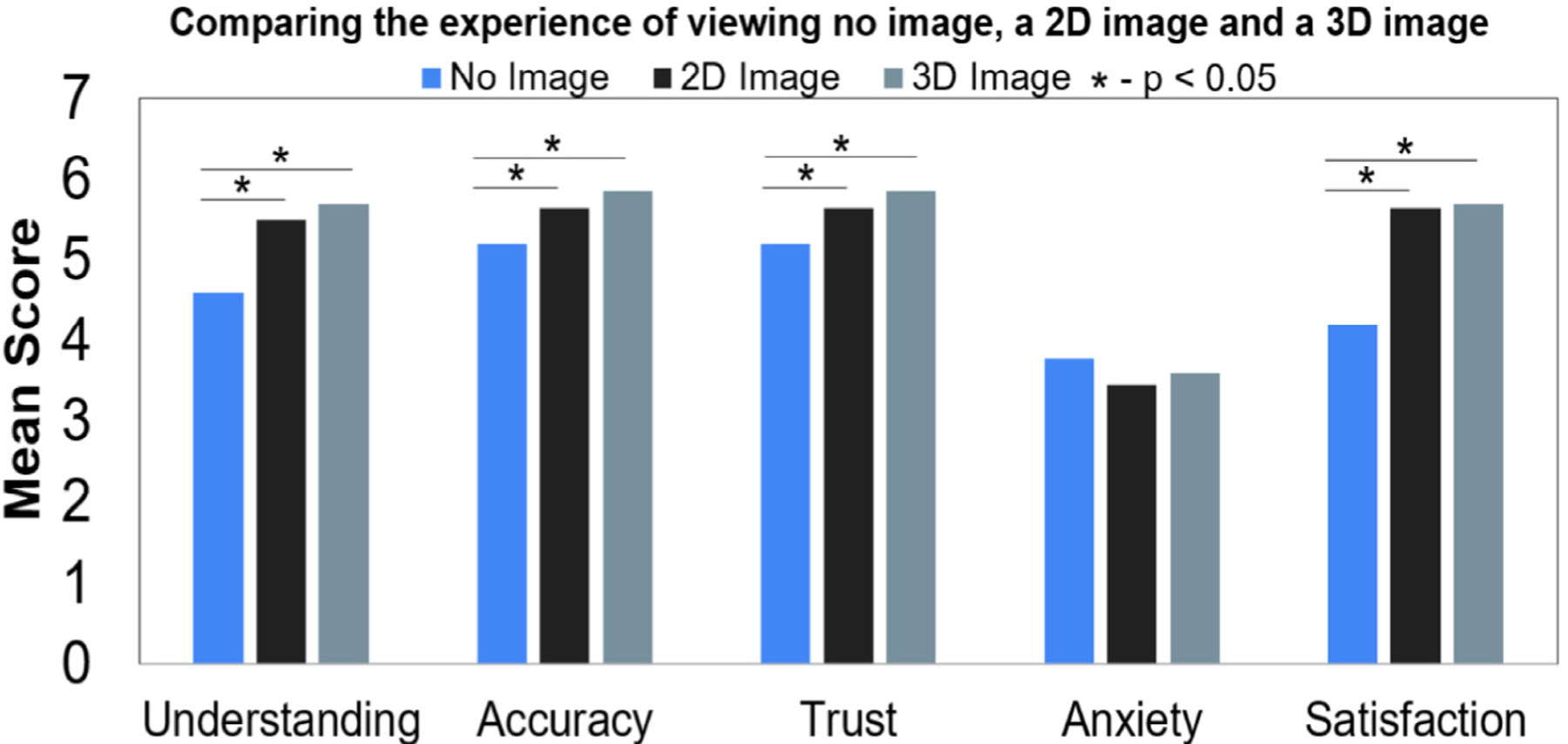
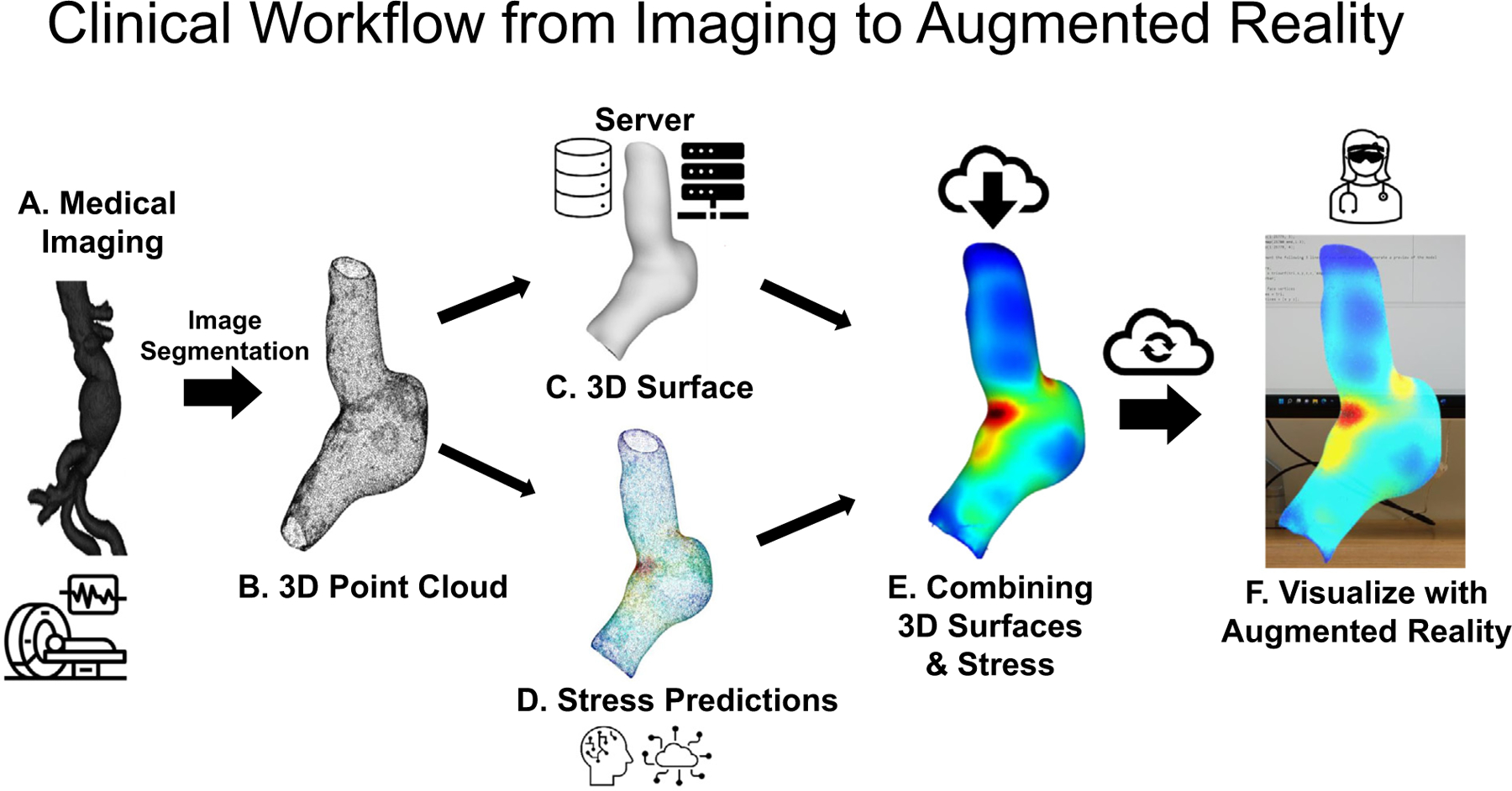
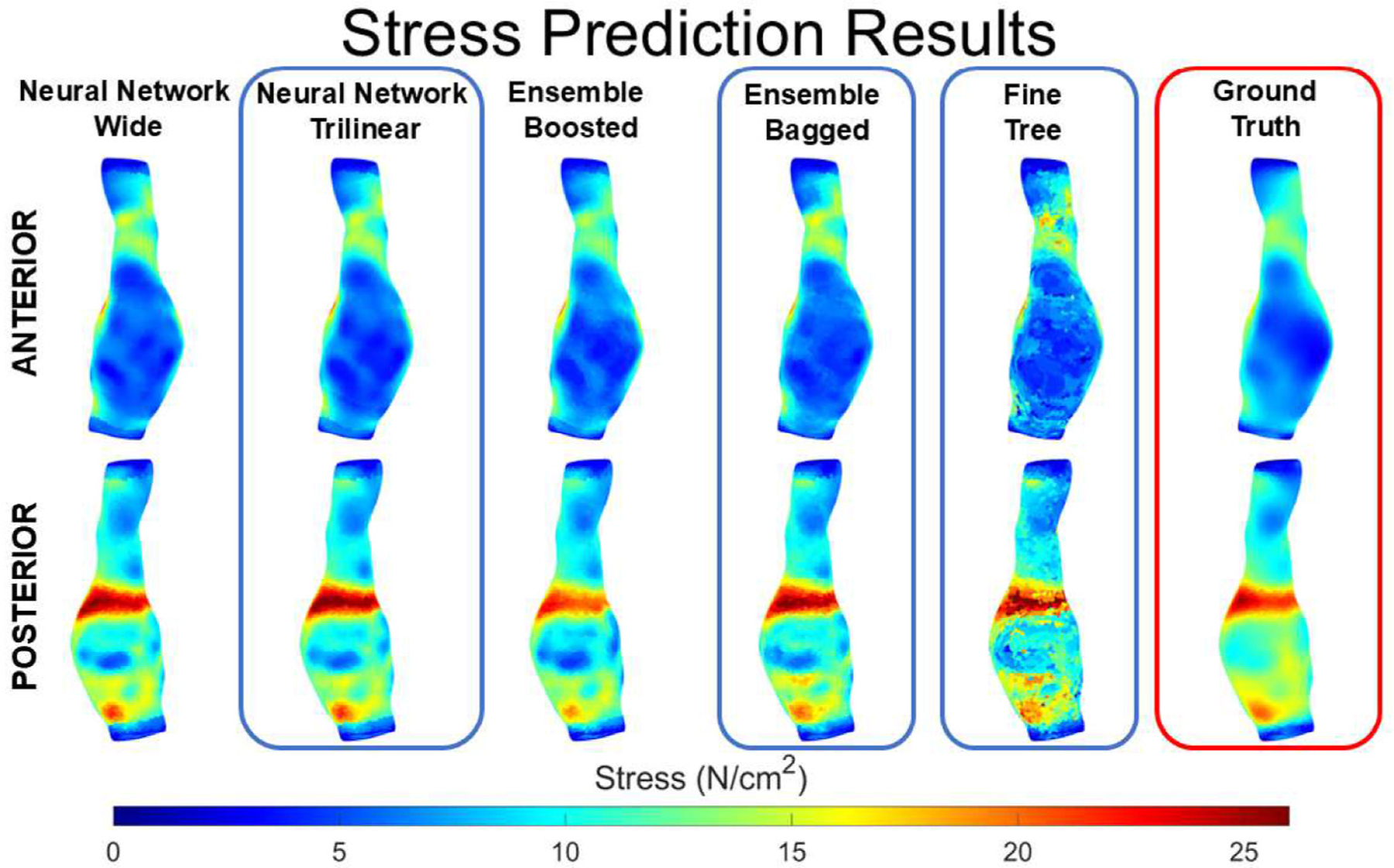
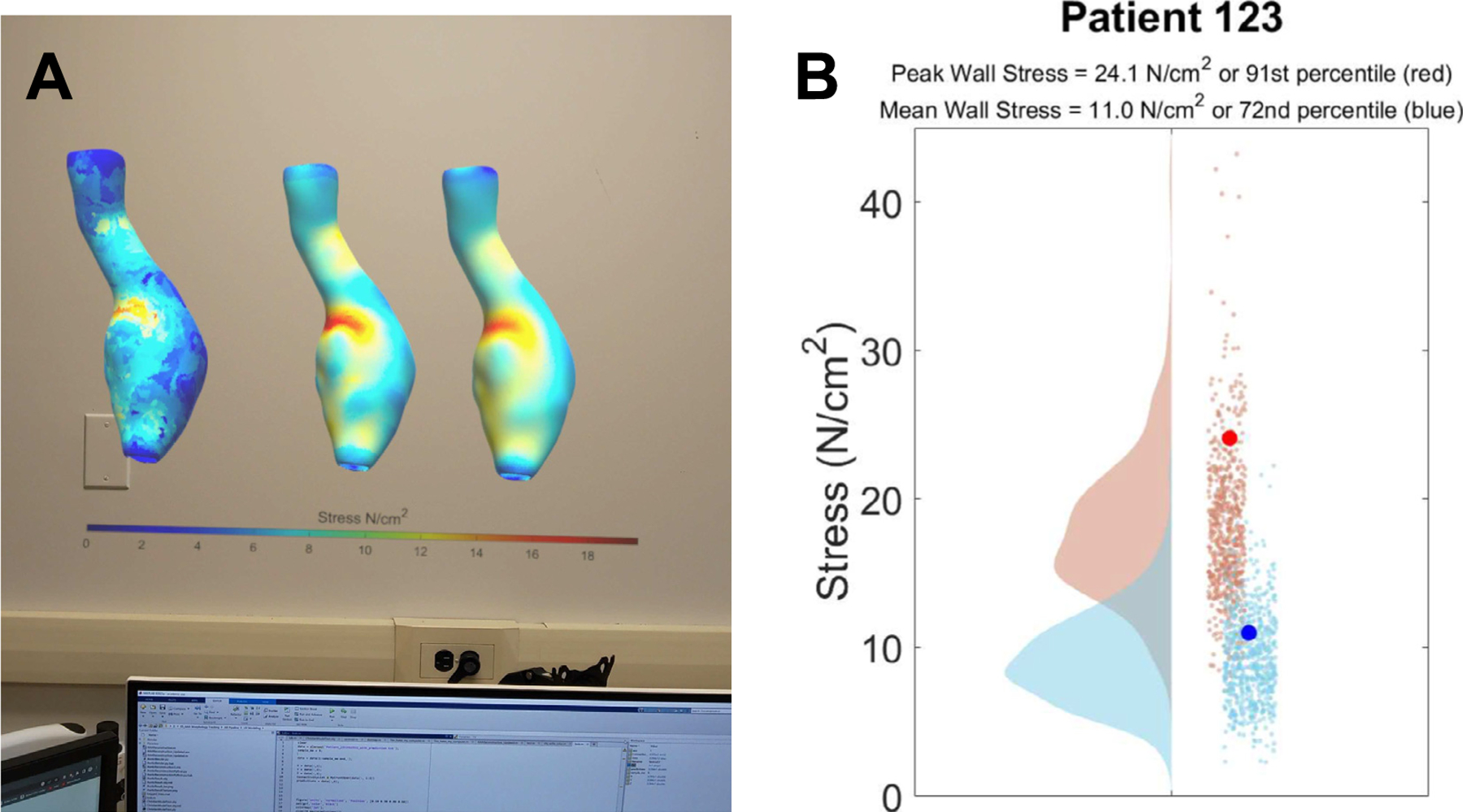
The number of medical images taken has continued to increase year over year for an aging population in the United States. It has been shown that patients understand their diagnoses better when shown a 2D or 3D image of their respective diseases. However, clinicians do not regularly show patients their images as it requires additional time and processing. In this experiment, we demonstrate the use of augmented reality to visualize abdominal aortic aneurysms using a previously developed artificial intelligence engine. Our group further expanded the number of cases used for training the stress prediction model to a total of 274 patients (206 used for training or ~ 5.4 million nodes, and 68 for testing or ~1.8 million nodes). Medical images undergo automated segmentation, and wall stresses are predicted on the 3D surface of aneurysms to view a heat map. The pipeline includes introducing elements into the Microsoft HoloLens 2 ecosystem to view models and additional analytics, enabling clinicians and patients to view the biomechanical status without the need for a computational or imaging expert. The proposed clinical workflow would allow a local server to process medical imaging data, generate point clouds, predict wall stresses on individual points, and create a 3D model with a colormap to view in augmented reality. The study revealed that neural networks and ensemble boosted tress models predicted the wall stresses more accurately (when compared to ground truth finite element analysis results). The approach is not limited to the HoloLens 2 ecosystem but can be used with other emerging augmented or virtual reality hardware systems.
Keywords: Abdominal aortic aneurysms; Artificial intelligence; Augmented reality; Biomechanics; Metaverse; Stress analysis; Visualization.
Figures
Similar articles
-
Nextmed: Automatic Imaging Segmentation, 3D Reconstruction, and 3D Model Visualization Platform Using Augmented and Virtual Reality.Sensors (Basel). 2020 May 23;20(10):2962. doi: 10.3390/s20102962. Sensors (Basel). 2020. PMID: 32456194 Free PMC article.
-
Navigation and visualisation with HoloLens in endovascular aortic repair.Innov Surg Sci. 2018 Oct 4;3(3):167-177. doi: 10.1515/iss-2018-2001. eCollection 2018 Sep. Innov Surg Sci. 2018. PMID: 31579781 Free PMC article.
-
Artificial intelligence framework to predict wall stress in abdominal aortic aneurysm.Appl Eng Sci. 2022 Jun;10:100104. doi: 10.1016/j.apples.2022.100104. Epub 2022 May 2. Appl Eng Sci. 2022. PMID: 37711641 Free PMC article.
-
Metaverse-based simulation: a scoping review of charting medical education over the last two decades in the lens of the 'marvelous medical education machine'.Ann Med. 2024 Dec;56(1):2424450. doi: 10.1080/07853890.2024.2424450. Epub 2024 Nov 13. Ann Med. 2024. PMID: 39535116 Free PMC article.
-
From static web to metaverse: reinventing medical education in the post-pandemic era.Ann Med. 2024 Dec;56(1):2305694. doi: 10.1080/07853890.2024.2305694. Epub 2024 Jan 23. Ann Med. 2024. PMID: 38261592 Free PMC article. Review.
Cited by
-
Artificial intelligence-based machine learning protocols enable quicker assessment of aortic biomechanics: A case study.J Vasc Surg Cases Innov Tech. 2025 Apr 14;11(4):101806. doi: 10.1016/j.jvscit.2025.101806. eCollection 2025 Aug. J Vasc Surg Cases Innov Tech. 2025. PMID: 40488185 Free PMC article.
References
-
- [1] Darling RC, Messina CR, Brewster DC, Ottinger LW, Autopsy study of unoperated abdominal aortic aneurysm s. the case for early resection, Circulation 56 (1977) II161–II164. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources