

Global, regional, and national burden of cardiovascular disease attributable to high body mass index from 1990 to 2021 and projection to 2045
- PMID: 40357206
- PMCID: PMC12066273
- DOI: 10.3389/fendo.2025.1546176
Global, regional, and national burden of cardiovascular disease attributable to high body mass index from 1990 to 2021 and projection to 2045
Abstract
Background: High body mass index (HBMI) is strongly associated with cardiovascular disease (CVD), but the global burden of CVD attributable to HBMI remains poorly defined. This study aims to elucidate the current burden and temporal trends of CVD attributable to HBMI.
Methods: We used data from the Global Burden of Disease Study (GBD) 2021 to estimate CVD deaths and disability-adjusted life years (DALYs) attributable to HBMI. Our analysis examines trends in deaths and DALYs by age, gender, and Socio-demographic Index (SDI) across global, regional, and national levels from 1990 to 2021. We used health inequality and decomposition analyses to quantify the influencing factors of disease burden and a Bayesian age-period-cohort (BAPC) model to predict the potential trend of HBMI on CVD burden.
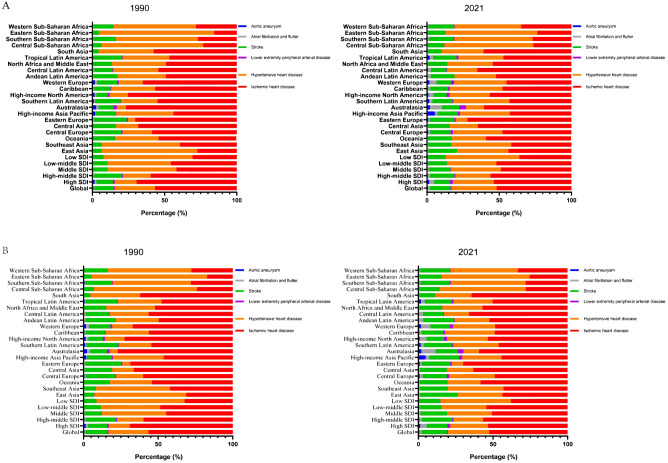
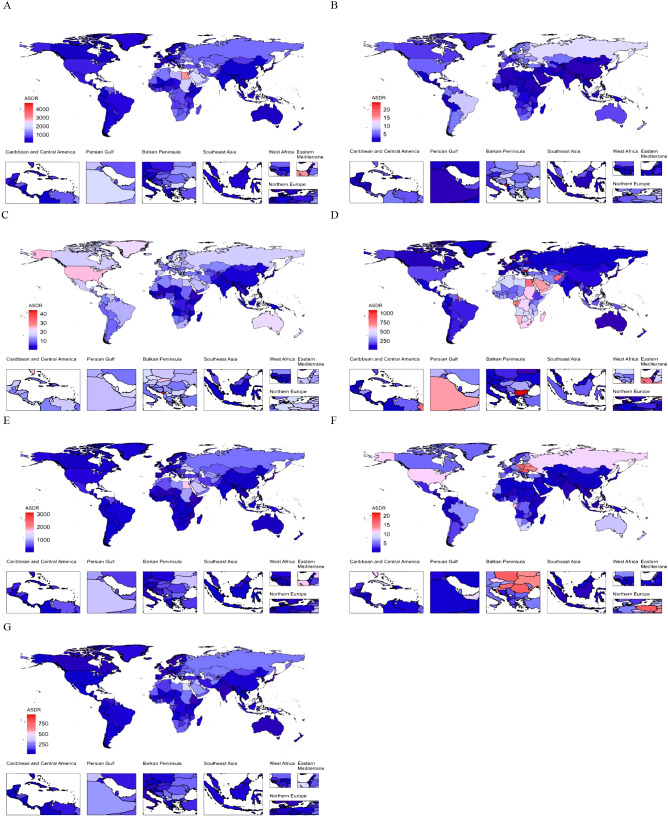
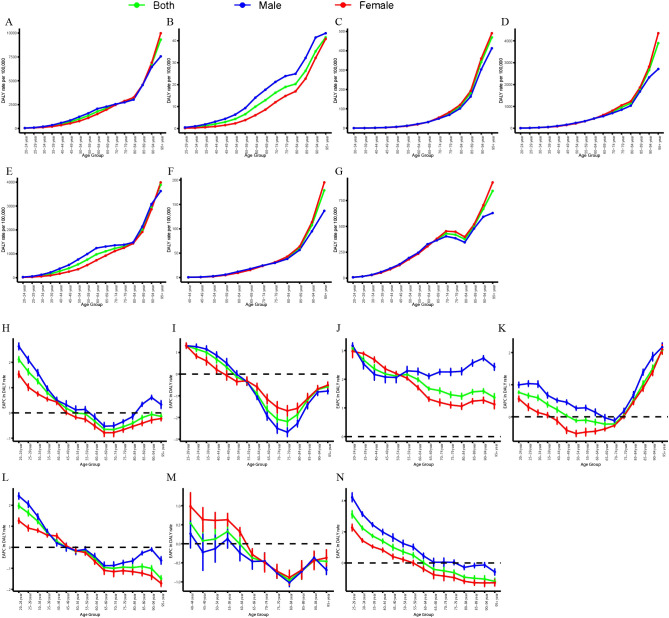
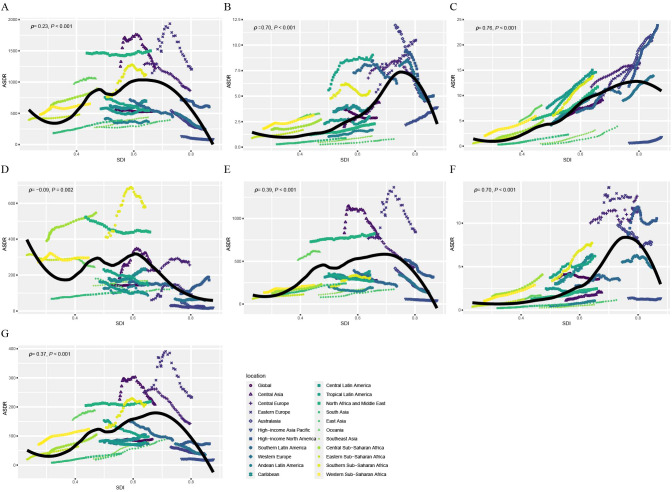
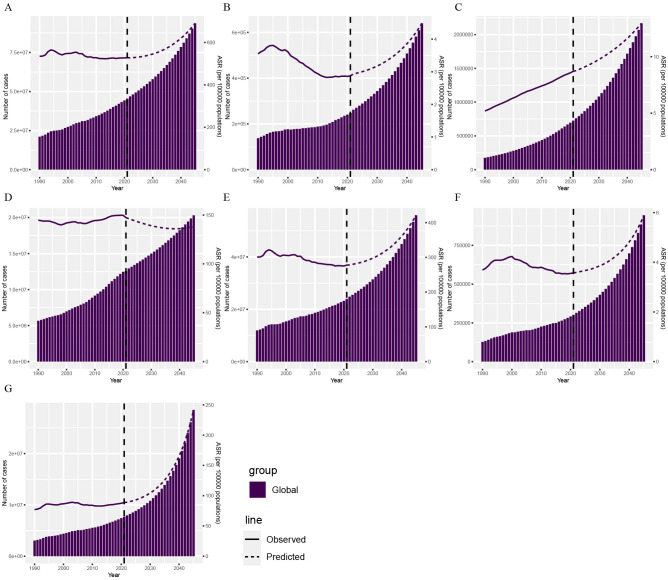
Results: In 2021, HBMI-related CVD resulted in approximately 1.9 million deaths and 45.43 million DALYs among urban and rural populations, with an age-standardized mortality rate (ASMR) of 22.77 (95% UI, 12.87-34.24) and an age-standardized disability rate (ASDR) of 529.00 (95% UI, 277.28-808.64) per 100,000 people. Over the study period, the overall CVD burden attributable to HBMI decreased significantly, while the burden of atrial fibrillation and flutter increased. The disease burden was closely tied to socioeconomic development and was unevenly distributed, with middle SDI regions experiencing a heavier burden. The highest burden was observed in individuals aged 84 and older, with a significant increase in the 20-44 age group. Decomposition analysis revealed that the increase in DALYs was driven by population growth. Projections from the BAPC model suggest that by 2045, global DALYs of CVD attributable to HBMI may continue to increase.
Conclusions: This study provides a comprehensive epidemiological assessment of the CVD burden attributable to HBMI across various regions and populations, offering valuable insights for guiding policy and research efforts.
Keywords: cardiovascular disease; epidemiology; global burden of disease; high body mass index; public health.
Copyright © 2025 Li, Liang, Song and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Global trend and disparity in the burden of thyroid cancer attributable to high body-mass index from 1990 to 2021 and projection to 2049: a systematic analysis based on the Global Burden of Disease Study 2021.BMC Public Health. 2025 Mar 18;25(1):1051. doi: 10.1186/s12889-025-21960-9. BMC Public Health. 2025. PMID: 40102768 Free PMC article.
-
The burden of cardiovascular disease attributable to high body mass index-an observational study.Eur Heart J Qual Care Clin Outcomes. 2024 Mar 1;10(2):154-167. doi: 10.1093/ehjqcco/qcad044. Eur Heart J Qual Care Clin Outcomes. 2024. PMID: 37481694
-
Trends and predictions of the global burden of ischemic heart disease in women of childbearing age attribute to high body mass index and hypertension,1990-2021: a systematic analysis for the Global Burden of Disease Study.BMC Cardiovasc Disord. 2025 May 9;25(1):360. doi: 10.1186/s12872-025-04741-5. BMC Cardiovasc Disord. 2025. PMID: 40346517 Free PMC article.
-
Global burden, risk factors, and projections of early-onset dementia: Insights from the Global Burden of Disease Study 2021.Ageing Res Rev. 2025 Feb;104:102644. doi: 10.1016/j.arr.2024.102644. Epub 2024 Dec 17. Ageing Res Rev. 2025. PMID: 39701185 Review.
-
Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study.J Am Coll Cardiol. 2020 Dec 22;76(25):2982-3021. doi: 10.1016/j.jacc.2020.11.010. J Am Coll Cardiol. 2020. PMID: 33309175 Free PMC article. Review.
References
-
- Singh-Manoux A, Fayosse A, Sabia S, Tabak A, Shipley M, Dugravot A, et al. . Clinical, socioeconomic, and behavioural factors at age 50 years and risk of cardiometabolic multimorbidity and mortality: A cohort study. PloS medicine. (2018) 15:e1002571. doi: 10.1371/journal.pmed.1002571 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical