

Organoid morphology-guided classification for oral cancer reveals prognosis
- PMID: 40359934
- PMCID: PMC12147898
- DOI: 10.1016/j.xcrm.2025.102129
Organoid morphology-guided classification for oral cancer reveals prognosis
Abstract
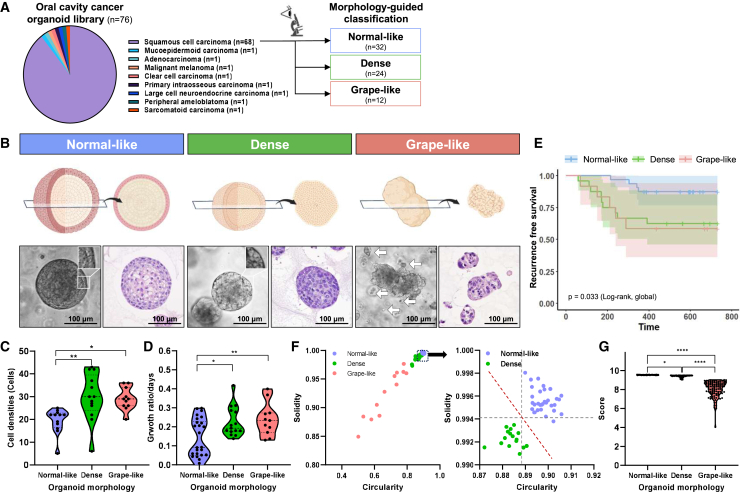
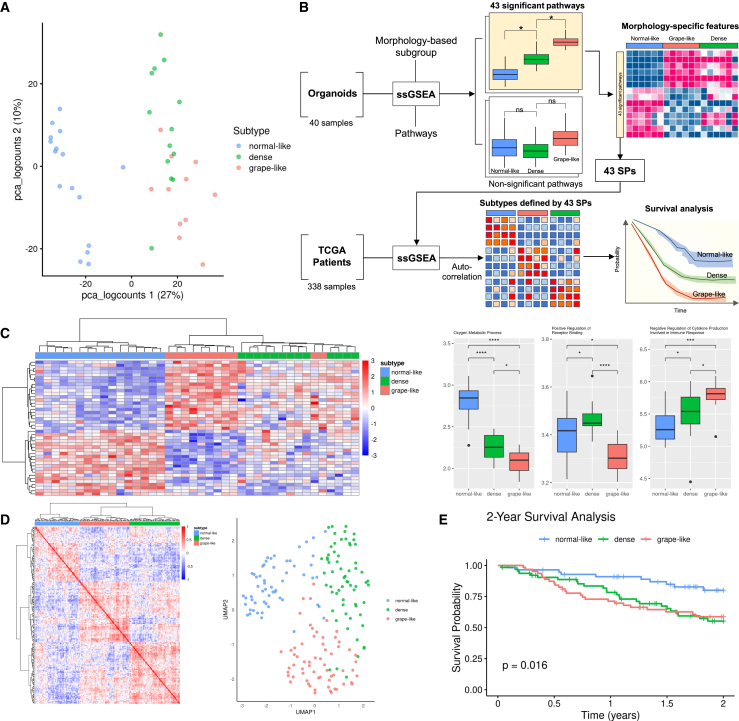
Oral cancer is an aggressive malignancy with a survival rate below 50% in advanced stages due to low mutation rates, lack of molecular subtypes, and limited treatment targets. This study presents a pioneering approach to classifying oral cancer subtypes based on the morphology of patient-derived organoids (PDOs) and proposes a therapeutic strategy. We establish 76 cancer and 81 normal PDOs. For cancer PDOs, both manual classification and AI-based scoring are utilized to categorize them into three distinct subtypes: normal-like, dense, and grape-like. These subtypes correlate with unique transcriptomic profiles, genetic mutations, and clinical outcomes, with patients harboring dense and grape-like organoids exhibiting poorer prognoses. Furthermore, drug response assessments of 14 single agents and cisplatin combination therapies identify a synergistic treatment approach for resistant subtypes. This study highlights the potential of integrating morphology-based classification with genomic and transcriptomic analyses to refine oral cancer subtyping and develop effective treatment strategies.
Keywords: combination therapy; morphology analysis; oral cancer; organoids.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures




References
-
- Abrahao R., Anantharaman D., Gaborieau V., Abedi-Ardekani B., Lagiou P., Lagiou A., Ahrens W., Holcatova I., Betka J., Merletti F., et al. The influence of smoking, age and stage at diagnosis on the survival after larynx, hypopharynx and oral cavity cancers in Europe: The ARCAGE study. Int. J. Cancer. 2018;143:32–44. doi: 10.1002/ijc.31294. - DOI - PubMed
-
- Choi Y.S., Kim M.G., Lee J.H., Park J.Y., Choi S.W. Analysis of prognostic factors through survival rate analysis of oral squamous cell carcinoma patients treated at the National Cancer Center: 20 years of experience. J. Korean Assoc. Oral Maxillofac. Surg. 2022;48:284–291. doi: 10.5125/jkaoms.2022.48.5.284. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
