

High flow nasal therapy versus noninvasive ventilation for AECOPD with acute hypercapnic respiratory failure: a meta-analysis of randomized controlled trials
- PMID: 40360910
- PMCID: PMC12075079
- DOI: 10.1186/s13613-025-01480-w
High flow nasal therapy versus noninvasive ventilation for AECOPD with acute hypercapnic respiratory failure: a meta-analysis of randomized controlled trials
Abstract
Background: Guidelines recommend the use of noninvasive ventilation (NIV) and high-flow nasal cannula (HFNC) in patients with chronic obstructive pulmonary disease (COPD) and hypercapnic acute respiratory failure (ARF). It is unclear whether HFNC is noninferior to NIV in terms of the rate of tracheal intubation or mortality. This meta-analysis aimed to compare the efficacy of HFNC and NIV in patients with AECOPD and hypercapnic ARF.
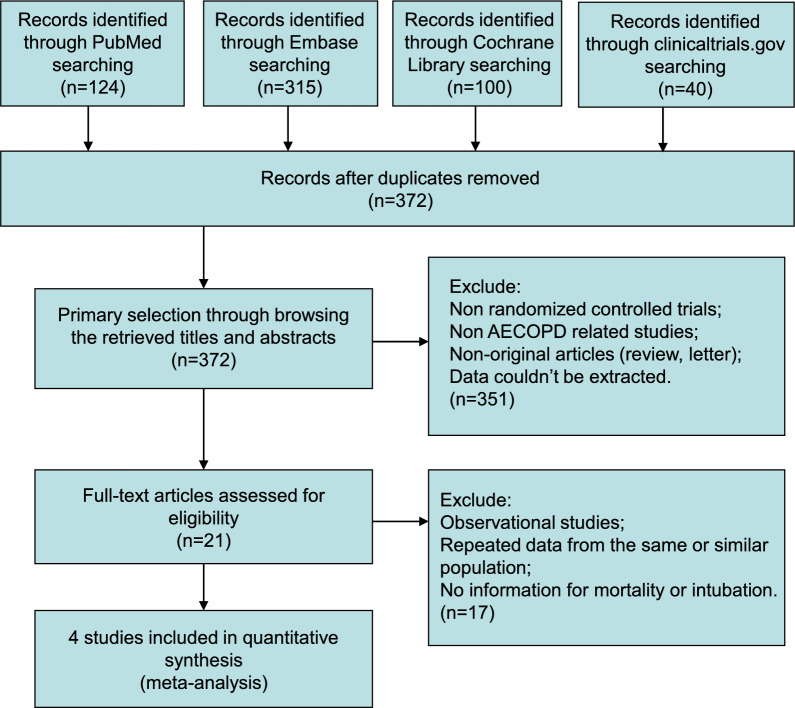
Methods: A systematic search was made of PubMed, Embase, Cochrane Library, and clinicaltrials.gov, without language restrictions. Randomized controlled trials (RCTs) on treatment of hypercapnic AECOPD with HFNC, compared with NIV, were reviewed. Estimated effects of included studies were pooled as risk ratios (RRs), with 95% confidence intervals (CIs).
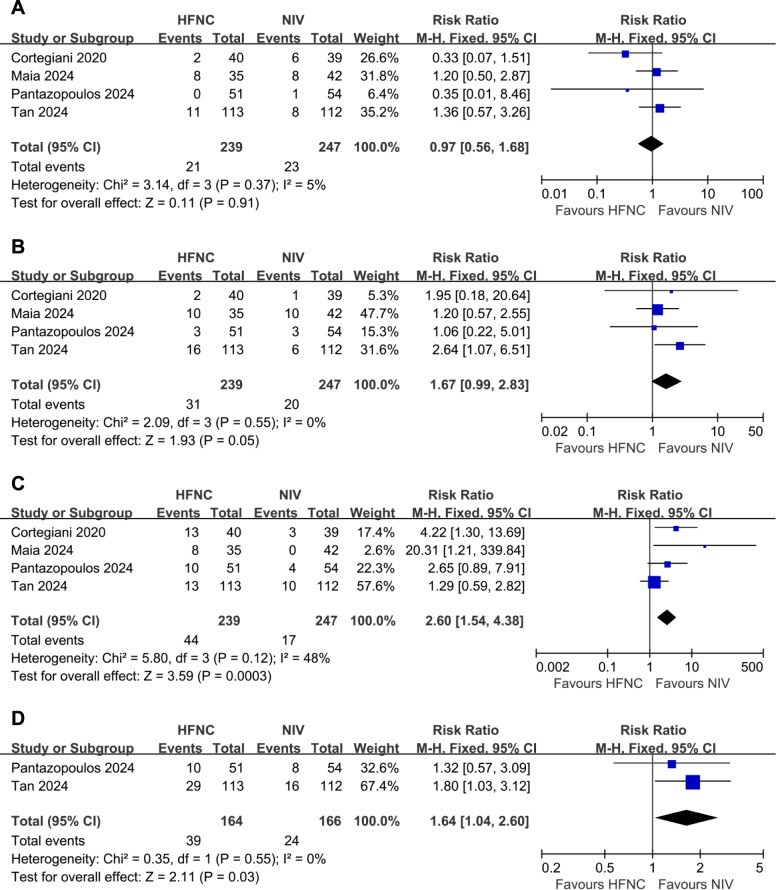
Results: Four RCTs (enrolling 486 patients) met the inclusion criteria. There was no statistically significant difference in all-cause mortality (RR 0.97, 95% CI 0.56 to 1.68), and intubation rate (RR 1.67, 95% CI 0.99 to 2.83) between the two groups. The treatment switch rate (RR 2.60, 95% CI 1.54 to 4.38) and treatment failure rate (RR 1.64, 95% CI 1.04 to 2.60) were significantly lower in NIV groups.
Conclusions: Compared with NIV, HFNC was not associated with increased mortality and intubation rate. More patients receiving HFNC oxygen therapy experienced treatment failure and switched to NIV, which may mask the fact that HFNC is inferior to NIV in patients with AECOPD and hypercapnic ARF.
Keywords: COPD; HFNC; Mortality; NIV.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: None of the authors has a competing interests to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
