

Thoracic CT Angiographies in Children Using Automated Power Injection with Bolus Tracking Versus Manual Contrast Injection: Analysis of Contrast Enhancement, Image Quality and Radiation Exposure
- PMID: 40361921
- PMCID: PMC12071457
- DOI: 10.3390/diagnostics15091103
Thoracic CT Angiographies in Children Using Automated Power Injection with Bolus Tracking Versus Manual Contrast Injection: Analysis of Contrast Enhancement, Image Quality and Radiation Exposure
Abstract
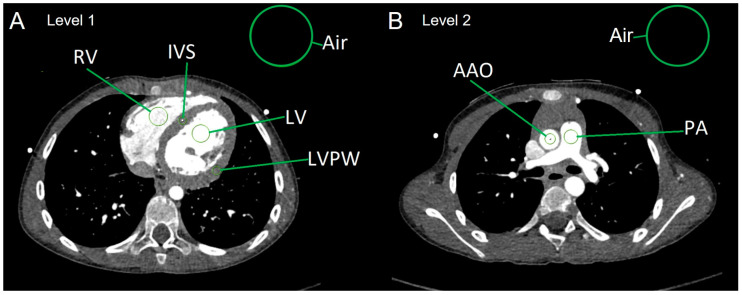
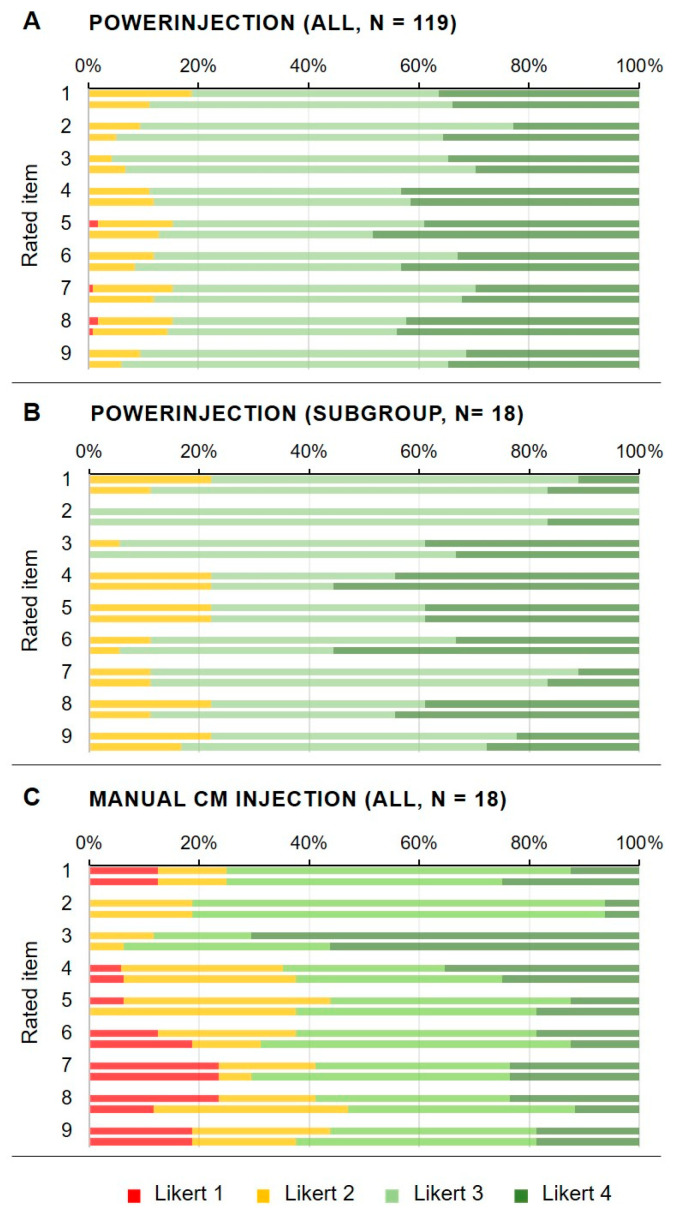
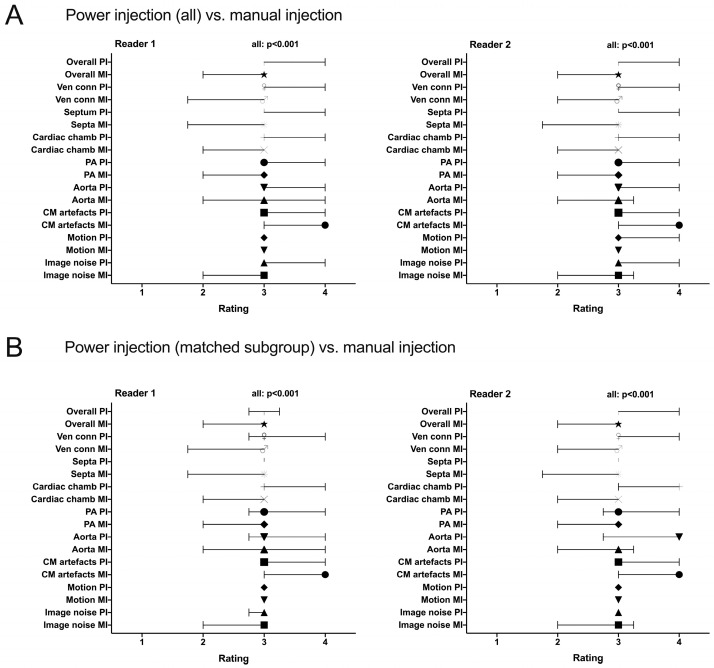
Objectives: The purpose of this study was to analyze image quality and radiation exposure of thoracic computed tomography angiography (CTA) in children with congenital heart diseases (CHDs) using either manual contrast medium (CM) injection or automated power injectors with bolus tracking. Methods: A total of 137 thoracic CTAs of 120 consecutive pediatric patients were included in this retrospective study. We analyzed the method of CM administration (power injection with bolus tracking (PI) or manual injection (MI)), injection routes, volumes and flow rates of CM. For the evaluation of objective image quality, attenuation values in the heart chambers and great thoracic vessels were determined by region-of-interest (ROI) analysis and signal-to-noise (SNR) and contrast-to-noise (CNR) ratios calculated thereof. Visual image quality was assessed by two blinded readers (four-point Likert-scale) analyzing the presence of artifacts and the depiction of relevant anatomical structures. Effective radiation doses were calculated with dose length products and specific conversion factors. Results: CM administration was performed using PI in 119/137 CTAs, whereas MI was conducted in 18/137. The smallest size of peripheral venous cannulas was 24 gauge in 36/137 (26.3%) cases. Overall mean CM volume was 17 mL ± 16 mL (mean ± SD). In PI, the mean flow rate of CM was 1.52 ± 0.90 mL/s with a range between 0.5 and 5.0 mL/s. When comparing the overall PI population and an age-, size- and weight-matched PI subpopulation (18 cases) with the MI population, attenuation values in Hounsfield units (HU) and CNR values were significantly higher in the PI groups than in the MI group for each relevant cardiac structure (left ventricle, right ventricle, ascending aorta and pulmonary trunk, p = 0.02-0.001). Overall image quality and depiction of cardiac structures were rated significantly better in CTAs with PI (interquartile ranges: "good" to "excellent" (Likert 3-4)) in PI compared with CTAs acquired with MI (interquartile ranges: "fair" to "good" (2-3)) in MI by both readers (p < 0.001). The inter-observer reliability was strong, with a Kendall's Tau-b correlation coefficient of τ = 0.802 (p < 0.001). The mean effective radiation dose (E) did not differ significantly when comparing the stratified samples (i.e., the matched PI subgroup and the MI group; 0.5 (±0.3) mSv in both, p = 0.76). There were no complications associated with the CM injections for both application approaches. Conclusions: Automated contrast agent applications with power injectors and bolus tracking ensure better image quality in pediatric CTA, even when low volumes and flow rates need to be applied. There is a slight increase in radiation associated with bolus tracking. This approach represents a suitable imaging technique for the work-up of congenital heart disease.
Keywords: automated power injector; bolus tracking; computed tomography angiography; congenital heart disease; contrast medium; image quality; manual injection.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Comparison of Power Versus Manual Injection in Bolus Shape and Image Quality on Contrast-Enhanced Magnetic Resonance Angiography: An Experimental Study in a Swine Model.Invest Radiol. 2017 Sep;52(9):547-553. doi: 10.1097/RLI.0000000000000383. Invest Radiol. 2017. PMID: 28448310
-
Contrast medium injection optimisation in spiral CT for the diagnosis of pulmonary embolism.Radiol Med. 2003 May-Jun;105(5-6):416-24. Radiol Med. 2003. PMID: 12949452 English, Italian.
-
Contrast medium application in pediatric high-pitch cardiovascular CT angiography: manual or power injection?J Cardiovasc Comput Tomogr. 2014 Jul-Aug;8(4):315-22. doi: 10.1016/j.jcct.2014.05.002. Epub 2014 May 22. J Cardiovasc Comput Tomogr. 2014. PMID: 25017867
-
Cardiac CT in the Preoperative Diagnostics of Neonates with Congenital Heart Disease: Radiation Dose Optimization by Omitting Test Bolus or Bolus Tracking.Acad Radiol. 2020 May;27(5):e102-e108. doi: 10.1016/j.acra.2019.07.019. Epub 2019 Aug 20. Acad Radiol. 2020. PMID: 31444109
-
Feasibility of a Single Contrast Bolus High-Pitch Pulmonary CT Angiography Protocol Followed by Low-Dose Retrospectively ECG-Gated Cardiac CT in Patients with Suspected Pulmonary Embolism.Rofo. 2018 Jun;190(6):542-550. doi: 10.1055/s-0044-100725. Epub 2018 Feb 1. Rofo. 2018. PMID: 29390229 English.
References
-
- Sachdeva R., Armstrong A.K., Arnaout R., Grosse-Wortmann L., Han B.K., Mertens L., Moore R.A., Olivieri L.J., Parthiban A., Powell A.J. Novel Techniques in Imaging Congenital Heart Disease: JACC Scientific Statement. J. Am. Coll. Cardiol. 2024;83:63–81. doi: 10.1016/j.jacc.2023.10.025. - DOI - PMC - PubMed
-
- Sachdeva R., Valente A.M., Armstrong A.K., Cook S.C., Han B.K., Lopez L., Lui G.K., Pickard S.S., Powell A.J., Bhave N.M., et al. ACC/AHA/ASE/HRS/ISACHD/SCAI/SCCT/SCMR/SOPE 2020 Appropriate Use Criteria for Multimodality Imaging During the Follow-Up Care of Patients with Congenital Heart Disease: A Report of the American College of Cardiology Solution Set Oversight Committee and Appropriate Use Criteria Task Force, American Heart Association, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Pediatric Echocardiography. J. Am. Soc. Echocardiogr. 2020;33:e1–e48. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
