

The Many Faces of the Angry Peritoneum
- PMID: 40361981
- PMCID: PMC12071784
- DOI: 10.3390/diagnostics15091163
The Many Faces of the Angry Peritoneum
Abstract
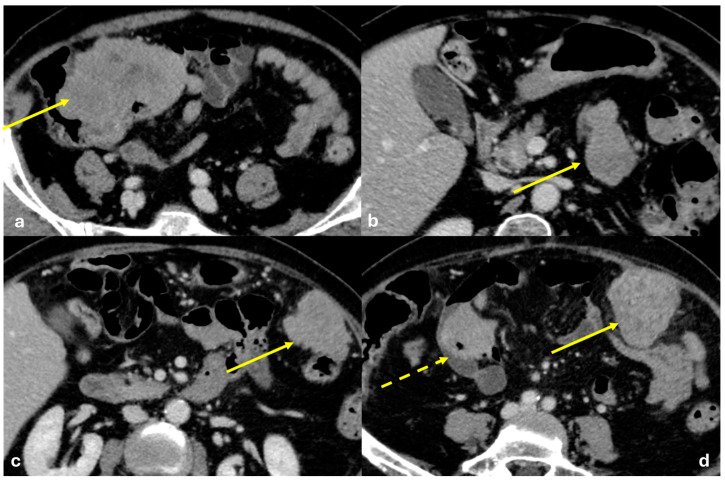
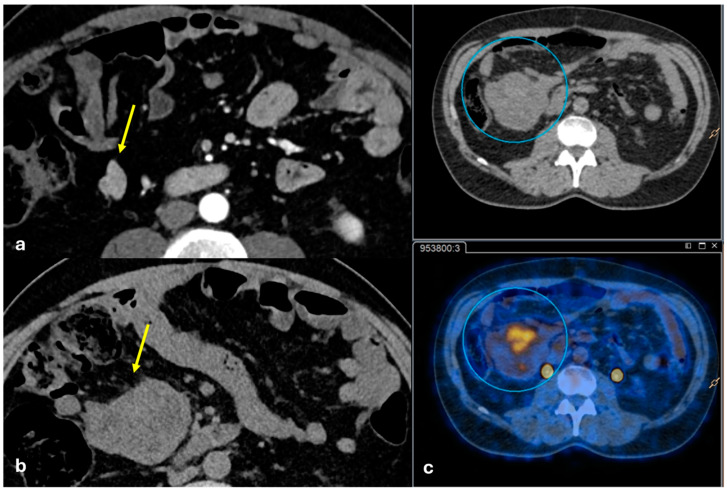
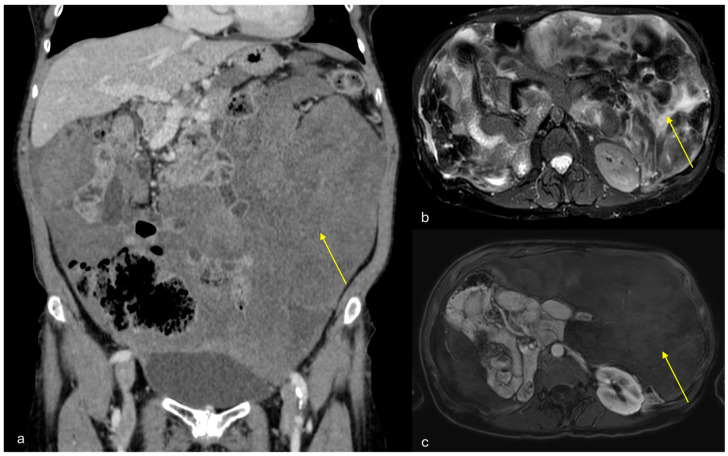
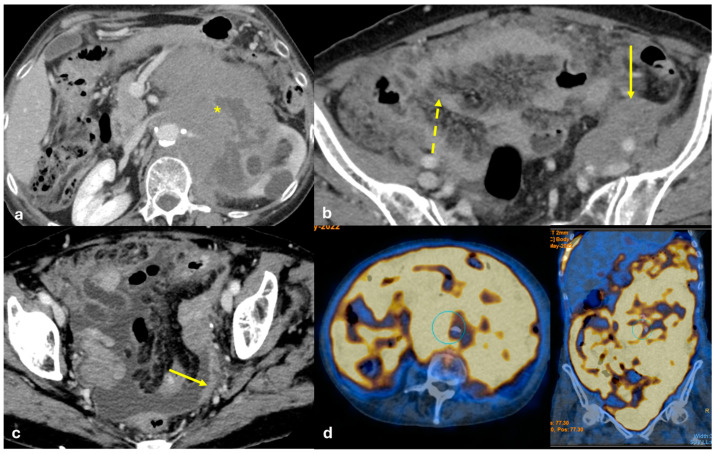
The peritoneum is a thin membrane that lines the abdominal cavity and covers the abdominal organs. It serves as a conduit for the spread of various pathological processes, including gas and fluid collections, inflammation, infections, and neoplastic conditions. Peritoneal carcinomatosis is the most common and well-known pathology involving the peritoneum, typically resulting from the dissemination of gastrointestinal and pelvic malignancies. However, numerous benign and malignant peritoneal diseases can mimic the imaging appearance of peritoneal carcinomatosis. The aim of this review is to revisit the anatomy of peritoneal compartments and elucidate the patterns of peritoneal disease spread. Emphasis is placed on identifying the distinctive imaging features of both neoplastic and non-neoplastic peritoneal diseases that differ from peritoneal carcinomatosis.
Keywords: disease pathways; peritoneal carcinomatosis; peritoneum.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
