

The Prevalence of Reduced Bone Mineral Density and the Impact of Specific Auxological Factors and Hormones on Bone Mass in Children with Endocrine Disorders
- PMID: 40364018
- PMCID: PMC12072271
- DOI: 10.3390/jcm14092988
The Prevalence of Reduced Bone Mineral Density and the Impact of Specific Auxological Factors and Hormones on Bone Mass in Children with Endocrine Disorders
Abstract
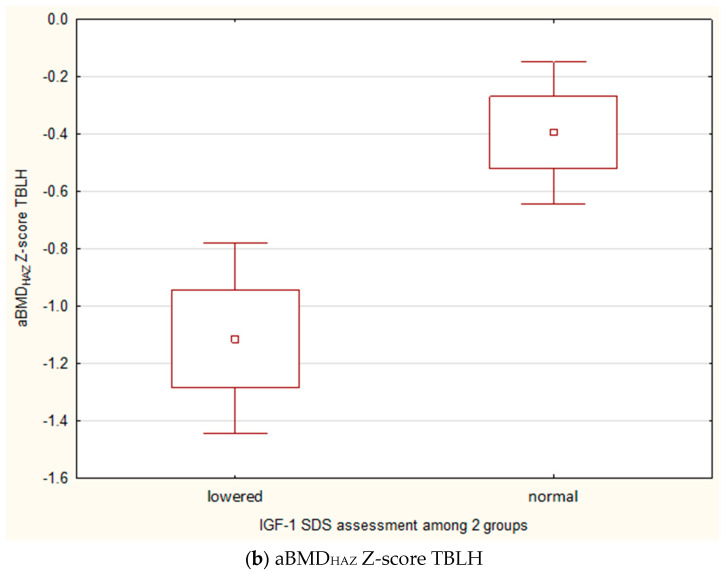
Background/Objectives: The skeletal system reaches peak bone mass through modeling and remodeling processes, influenced by environmental, dietary, hormonal, and genetic factors. In children with endocrinopathies, disturbances in bone mass and mineralization may correlate with hormonal levels, but conditions like short stature or obesity can confound DXA results. This study aimed to assess the prevalence of decreased bone mineral density (BMD) in children with endocrine disorders and evaluate the impact of auxological and hormonal abnormalities on BMD. Methods: This study analyzed medical records of 148 children (mean age 11.85 ± 3.34 years); 73 girls and 75 boys). Conditions included obesity (22.9%), short stature (47.9%), precocious puberty (10.1%), and other diagnoses. Clinical data included primary diagnosis, height, body weight, pubertal stage, and serum concentrations of calcium, phosphate, alkaline phosphatase, 25OHD, PTH, osteocalcin, Crosslaps, TSH, fT4, IGF-1, IGF-BP3, cortisol, estradiol, testosterone, and bone age. DXA scans were performed at the total body less head (TBLH) and lumbar spine (Spine) projection. Results: Low bone mass (aBMD Z-score ≤ -2) was found in 34.46% at TBLH and 15.54% at the Spine. After height adjustment (HAZ adjustment), the prevalence of low bone mass decreased to 11.4% at TBLH and 4.1% at the Spine. In the short stature group, the normalization of Z-scores for height significantly reduced abnormal results. A positive correlation was found between DXA parameters and age, height standard deviation score (HSDS), BMI SDS, estradiol, testosterone, IGF-1, and IGF-BP3. A negative correlation existed between vitamin D and DXA parameters. Bone turnover markers (osteocalcin and Crosslaps) also negatively affected bone mass. No significant correlations were found with PTH, TSH, fT4, or cortisol. In children with growth retardation, lower aBMDHAZ Z-scores were observed in those with decreased IGF-1. Positive correlations existed between BMI SDS, IGF-1, and adjusted aBMD Z-scores. Conclusions: Children with endocrine disorders, especially those with short stature, are at risk for bone mineralization disorders. Height normalization is crucial for accurate DXA interpretation and avoiding overdiagnosis. Positive influences on bone mass include height, BMI, IGF-1, estradiol, and testosterone, while negative factors include bone turnover markers and low vitamin D.
Keywords: IGF-1; bone mass; bone mineral density; children; dual X-ray densitometry; hormones.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






References
-
- Crabtree N.J., Arabi A., Bachrach L.K., Fewtrell M., El-Hajj Fuleihan G., Kecskemethy H.H., Jaworski M., Gordon C.M., International Society for Clinical Densitometry Dual-Energy X-Ray Absorptiometry Interpretation and Reporting in Children and Adolescents: The Revised 2013 ISCD Pediatric Official Positions. J. Clin. Densitom. 2014;17:225–242. doi: 10.1016/j.jocd.2014.01.003. - DOI - PubMed
-
- Zemel B.S., Leonard M.B., Kelly A., Lappe J.M., Gilsanz V., Oberfield S., Mahboubi S., Shepherd J.A., Hangartner T.N., Frederick M.M., et al. Height Adjustment in Assessing Dual Energy X-Ray Absorptiometry Measurements of Bone Mass and Density in Children. J. Clin. Endocrinol. Metab. 2010;95:1265–1273. doi: 10.1210/jc.2009-2057. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
