

Ct-Perfusion Absolute Ghost Infarct Core Is a Rare Phenomenon Associated with Poor Collateral Status in Acute Ischemic Stroke Patients
- PMID: 40364022
- PMCID: PMC12073032
- DOI: 10.3390/jcm14092991
Ct-Perfusion Absolute Ghost Infarct Core Is a Rare Phenomenon Associated with Poor Collateral Status in Acute Ischemic Stroke Patients
Abstract
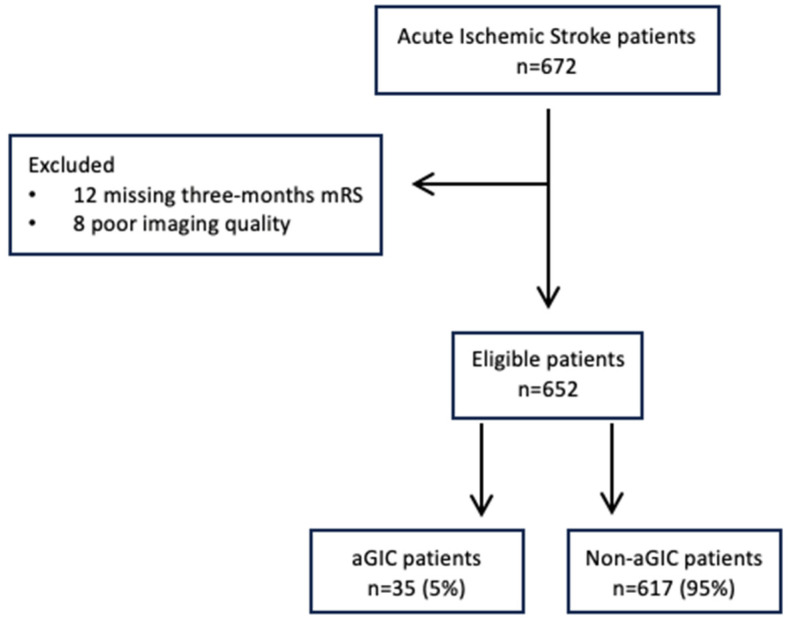
Background: CT perfusion (CTP) overestimation of core volume >10 mL compared to the final infarct volume (FIV) size is the current definition of the ghost infarct core (GIC) phenomenon. However, subsequent infarct growth might influence FIV. We aimed to report a more reliable assessment of GIC occurrence, defined as no evidence of infarct at 24 h follow-up imaging, compared to CTP core volume at admission. This phenomenon was named absolute GIC (aGIC), and we investigated its prevalence and predictors. Methods: A total of 652 consecutive stroke patients with large vessel occlusion who achieved successful recanalization (mTICI 2b-3) after endovascular treatment (EVT) and non-contrast CT (NCCT) follow-up imaging at 24 h were retrospectively analyzed. Ischemic core volume was automatically generated from CTP, and FIV was manually determined on follow-up NCCT. Multivariable logistic regression was used to explore aGIC predictors. Results: We included 652 patients (53.3% female, median age 75 years), of whom 35 (5.3%) had an aGIC. The aGIC group showed higher ASPECTS (p < 0.001), shorter (<3 h) onset-to-imaging time (p < 0.016), poorer collaterals (p < 0.001), and higher hypoperfusion intensity ratio (p < 0.001) compared to the non-aGIC group. In multivariate analysis, ASPECTS (odds ratio (OR), 2.37; p <0.001), onset-to-imaging time (OR, 0.99; p = 0.034), collateral score (OR, 0.24; p < 0.001), and hypoperfusion intensity ratio (OR, 23.2; p < 0.001) were independently associated with aGIC. Conclusions: aGIC is a more reliable evaluation of infarct core volume overestimation assessed on admission CTP and represents a rare phenomenon, associated with ultra-early presentation and poor collaterals.
Keywords: CT perfusion; absolute ghost infarct core; acute ischemic stroke; collaterals; endovascular treatment; large vessel occlusion.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Morotti declared consulting and expert meeting honoraria for EMG-REG International and AstraZeneca. Zini declared consulting and speaker fees from Boehringer-Ingelheim, Alexion-AstraZeneca and CSL Behring, Bayer, Angels Iniziative, and Daiichi-Sankio. All of the other authors report no disclosures.
Figures
References
-
- Albers G.W., Marks M.P., Kemp S., Christensen S., Tsai J.P., Ortega-Gutierrez S., McTaggart R.A., Torbey M.T., Kim-Tenser M., Leslie-Mazwi T., et al. DEFUSE 3 Investigators. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N. Engl. J. Med. 2018;378:708–718. doi: 10.1056/NEJMoa1713973. - DOI - PMC - PubMed
-
- Powers W.J., Rabinstein A.A., Ackerson T., Adeoye O.M., Bambakidis N.C., Becker K., Biller J., Brown M., Damaerschalk B.M., Hoh B., et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–e418. - PubMed
-
- Nogueira R.G., Jadhav A.P., Haussen D.C., Bonafe A., Budzik R.F., Bhuva P., Yavagal D.R., Ribo M., Cognard C., Hanel R.A., et al. DAWN Trial Investigators. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N. Engl. J. Med. 2018;378:11–21. doi: 10.1056/NEJMoa1706442. - DOI - PubMed
LinkOut - more resources
Full Text Sources
