

Cognitive Brain Networks and Enlarged Perivascular Spaces: Implications for Symptom Severity and Support Needs in Children with Autism
- PMID: 40364061
- PMCID: PMC12072625
- DOI: 10.3390/jcm14093029
Cognitive Brain Networks and Enlarged Perivascular Spaces: Implications for Symptom Severity and Support Needs in Children with Autism
Abstract
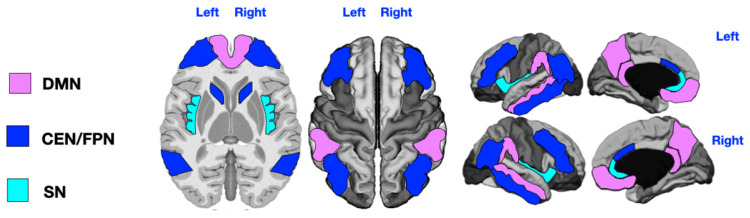
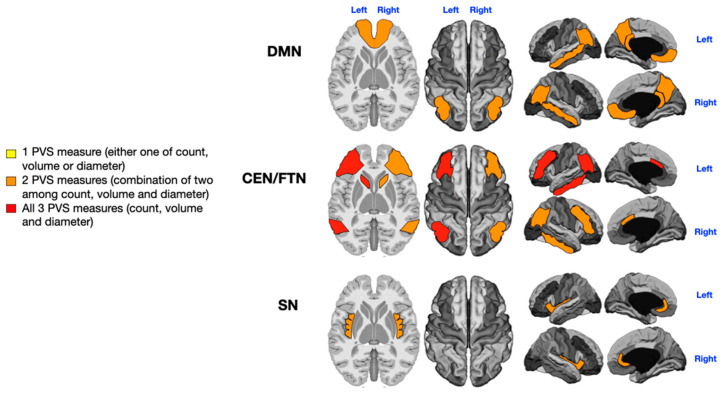
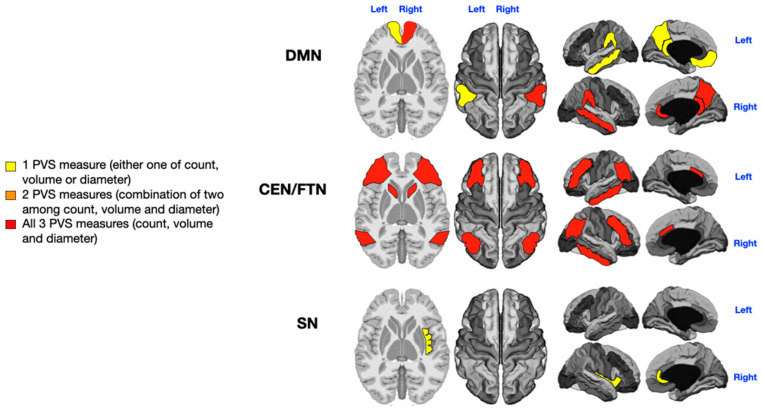
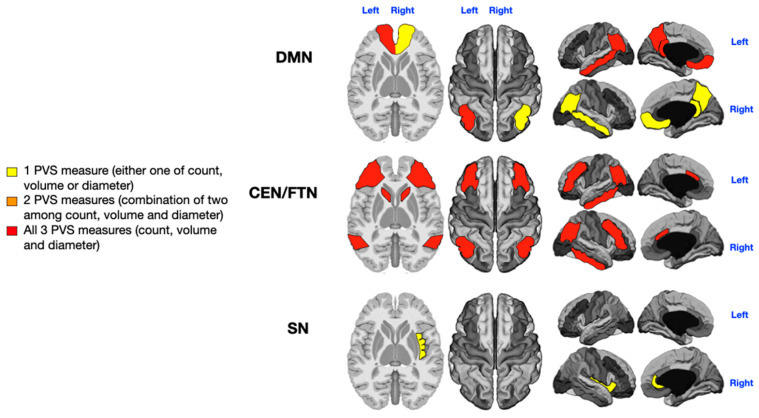
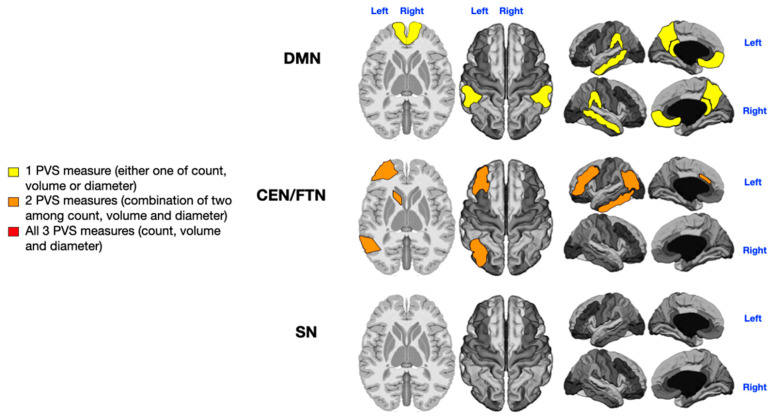
Background/Objectives: The severity of autism spectrum disorder (ASD) is clinically assessed through a comprehensive evaluation of social communication deficits, restricted interests, repetitive behaviors, and the level of support required (ranging from level 1 to level 3) according to DSM-5 criteria. Along with its varied clinical manifestations, the neuroanatomy of ASD is characterized by heterogeneous abnormalities. Notably, brain MRI of children with ASD often reveals an increased number of perivascular spaces (PVSs) compared to typically developing children. Our recent findings indicate that enlarged PVSs (ePVSs) are more common in younger male patients with severe ASD and that specific ePVS locations are significantly associated with ASD symptoms. Methods: In this study, we mapped ePVSs across key regions of three major cognitive networks-the Default Mode Network (DMN), the combined Central Executive/Frontoparietal Network (CEN/FPN), and the Salience Network (SN)-in 36 individuals with different symptom severities and rehabilitation needs due to ASD. We explored how the number, size, and location of PVSs in these networks are related to specific ASD symptoms and the overall need for rehabilitation and support. Results: Our results suggest that ePVSs in the DMN, CEN/FPN, and SN are strongly correlated with the severity of certain ASD symptoms, including verbal deficits, stereotypies, and sensory disturbances. We found a mild association between ePVSs and the level of support needed for daily living and quality of life. Conclusions: Dysfunction in cognitive networks associated with the presence of ePVSs has a significant impact on the severity of ASD symptoms. However, the need for assistance may also be influenced by other comorbid conditions and dysfunctions in smaller, overlapping brain networks.
Keywords: autism; brain functional networks; central executive network; default mode network; frontoparietal network; needs; perivascular spaces; salience network; symptoms.
Conflict of interest statement
The authors declare that there are no conflicts of interest that could prejudice the impartiality of the research reported.
Figures
References
-
- American Psychiatric Association aAPAD-TF . Diagnostic and Statistical Manual of Mental Disorders: DSM-5. American Psychiatric Association; Washington, DC, USA: 2013.
-
- McCrimmon A., Rostad K. Test Review: Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) Manual (Part II): Toddler Module. J. Psychoeduc. Assess. 2013;32:88–92. doi: 10.1177/0734282913490916. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
