

Association of a Left Atrial Diverticulum with Adverse Events During Catheter Ablation for Atrial Fibrillation
- PMID: 40364073
- PMCID: PMC12072600
- DOI: 10.3390/jcm14093041
Association of a Left Atrial Diverticulum with Adverse Events During Catheter Ablation for Atrial Fibrillation
Abstract
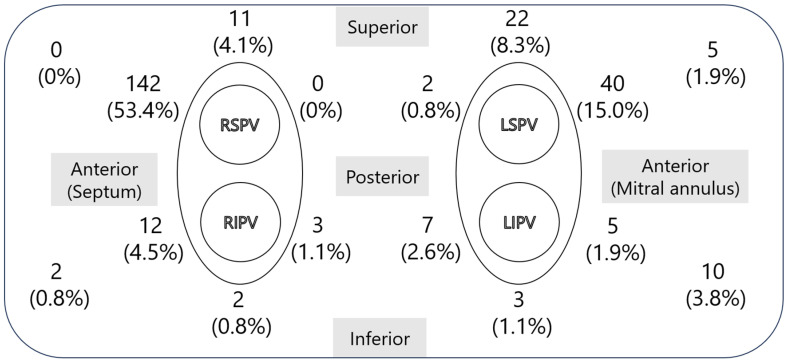
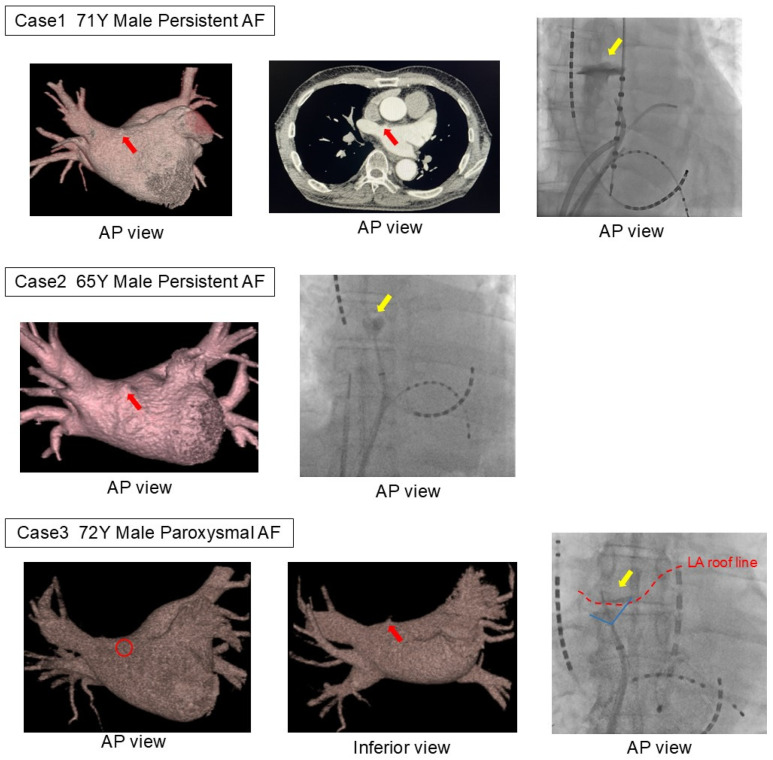
Background/Objectives: Left atrial diverticula (LADs) have been reported to potentially be associated with arrhythmic substrates, thromboembolic events, and complications during catheter ablation for atrial fibrillation (AF), but their clinical significance remains unclear. This study aimed to assess the prevalence, location, and potential relationship with complications during AF catheter ablation using preoperative CT. Methods: This study included 595 consecutive patients undergoing AF catheter ablation at Keio University Hospital from April 2021 to February 2024. Preoperative ECG-gated cardiac MDCT scans were analyzed to assess the presence and location of the LAD. Intraoperative adverse events were documented, and the association between the LAD and mechanical complications, such as a cardiac perforation and tamponade, was evaluated. Results: A total of 595 patients undergoing catheter ablation for AF or atrial tachycardia (AT) were included, with 210 (35.3%) found to have an LAD. No significant differences in age, sex, body mass index, or arrhythmia type were observed between patients with or without an LAD. LADs were most commonly located in the anterior region of the right superior pulmonary vein (53.4% of cases), followed by the anterior region of the left superior pulmonary vein (15% of cases). Perioperative complications occurred in 12 cases (2.0%), with 7 in the LAD group and 5 in the non-LAD group. Mechanical complications were observed exclusively in the LAD group (n = 4), with three of the cases associated with LADs. In all cases, LADs were present in the anterior region of the right superior pulmonary vein and were caused by the accidental insertion of an angiographic catheter into the LAD during pulmonary venography before insertion of the ablation catheter into the left atrium. However, all cases were hemodynamically stable, and the procedures were completed as planned. Conclusions: LADs are a more common anatomical structure than generally recognized and may be associated with mechanical complications during AF catheter ablation. Identifying the presence of an LAD on preoperative CT is crucial for predicting potential risks.
Keywords: atrial fibrillation; atrial tachycardia; cardiac computed tomography; catheter ablation; complications; left atrial diverticulum.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Peng L.Q., Yu J.Q., Yang Z.G., Wu D., Xu J.J., Chu Z.G., Li X.M., Chen D.D., Luo Y., Shao H., et al. Left atrial diverticula in patients referred for radiofrequency ablation of atrial fibrillation: Assessment of prevalence and morphologic characteristics by dual-source computed tomography. Circ. Arrhythm. Electrophysiol. 2012;5:345–350. doi: 10.1161/CIRCEP.111.965665. - DOI - PubMed
-
- Hołda M.K., Koziej M., Wszołek K., Pawlik W., Krawczyk-Ożóg A., Sorysz D., Łoboda P., Kuźma K., Kuniewicz M., Lelakowski J., et al. Left atrial accessory appendages, diverticula, and left-sided septal pouch in multi-slice computed tomography. Association with atrial fibrillation and cerebrovascular accidents. Int. J. Cardiol. 2017;244:163–168. doi: 10.1016/j.ijcard.2017.06.042. - DOI - PubMed
-
- Nagai T., Fujii A., Nishimura K., Inoue K., Suzuki J., Kido T., Nakamura M., Matsumoto Y., Izutani H., Mochizuki T., et al. Large thrombus originating from left atrial diverticulum: A new concern for catheter ablation of atrial fibrillation. Circulation. 2011;124:1086–1088. doi: 10.1161/CIRCULATIONAHA.110.000315. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
