

Critical Care Ultrasonography for Volume Management: A Systematic Review, Meta-Analysis, and Trial Sequential Analysis of Randomized Trials
- PMID: 40366291
- PMCID: PMC12080698
- DOI: 10.1097/CCE.0000000000001261
Critical Care Ultrasonography for Volume Management: A Systematic Review, Meta-Analysis, and Trial Sequential Analysis of Randomized Trials
Abstract
Objectives: To determine the safety and efficacy of critical care ultrasonography (CCUS) guided volume management in acutely ill patients.
Data sources: We searched MEDLINE, Embase, Wiley CENTRAL, and unpublished sources from inception to February 6, 2024.
Study selection: We included randomized controlled trials (RCTs) of acutely ill adult patients randomized to receive CCUS as compared with no CCUS to guide fluid management.
Data extraction: Reviewers screened abstracts, full texts, and extracted data independently and in duplicate. We pooled data using a random-effects model, assessed the risk of bias using the modified Cochrane tool and assessed the certainty of evidence using the Grading Recommendations Assessment, Development, and Evaluation approach.
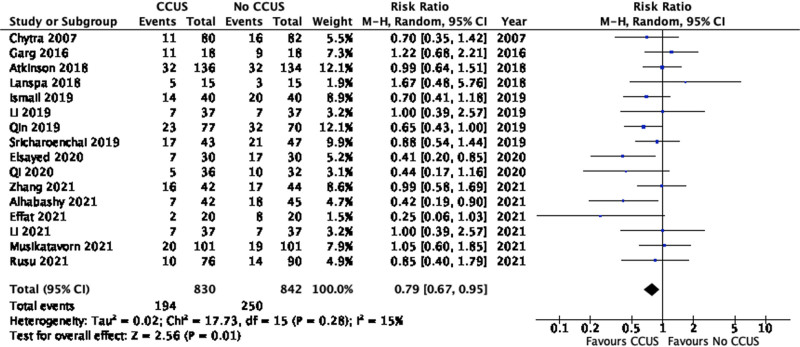
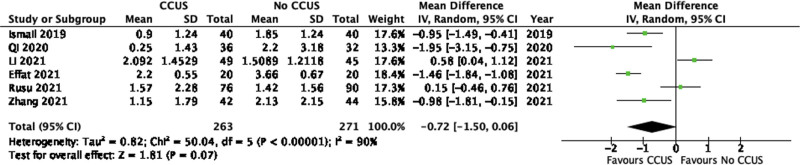
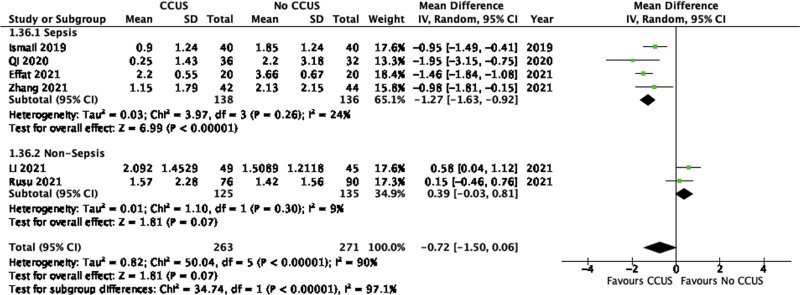
Data synthesis: We included 17 RCTs (n = 1765 patients) in this review. Pooled analyses found that the use of CCUS for volume management in acutely ill patients may decrease mortality at the longest reported time period (relative risk [RR], 0.79; 95% CI, 0.67-0.95; low certainty) and decreases the fluid balance up to 72 hours after admission (mean difference [MD], 0.72 L lower; 95% CI, 1.5 L lower to 0.07 L higher; low certainty). CCUS had an uncertain effect on duration of mechanical ventilation (MD, 1.14 d fewer; 95% CI, 3.35 d fewer to 1.07 d more; very low certainty), ICU length of stay (LOS) (MD, 0.01 d fewer; 95% CI, 1.12 d fewer to 1.09 d more; very low certainty), the need for vasopressors (RR, 0.39; 95% CI, 0.10-1.62; very low certainty), acute kidney injury (AKI) (RR, 0.94; 95% CI, 0.32-2.72; very low certainty), and the need for renal replacement therapy (RRT) (RR, 0.79; 95% CI, 0.17-3.66; very low certainty).
Conclusions: In acutely ill adult patients, CCUS for the use of targeted volume management may reduce mortality and fluid balance up to 72 hours after admission. CCUS has an uncertain effect on ICU LOS, duration of mechanical ventilation, duration of vasopressor use, AKI, and the need for RRT. However, this evidence is limited by imprecision and indirectness.
Keywords: critical care; point-of-care ultrasound; sepsis; ultrasound; volume overload.
Copyright © 2025 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Nikravan has received funds from Verathon. Dr. Sharif holds a McMaster University Department of Medicine Internal Career Research Award. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Boyd JH, Forbes J, Nakada TA, et al. : Fluid resuscitation in septic shock: A positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med 2011; 39:259–265 - PubMed
-
- Feissel M, Michard F, Faller JP, et al. : The respiratory variation in inferior vena cava diameter as a guide to fluid therapy. Intensive Care Med 2004; 30:1834–1837 - PubMed
-
- Monnet X, Rienzo M, Osman D, et al. : Passive leg raising predicts fluid responsiveness in the critically ill. Crit Care Med 2006; 34:1402–1407 - PubMed
-
- Bentzer P, Griesdale DE, Boyd J, et al. : Will this hemodynamically unstable patient respond to a bolus of intravenous fluids? JAMA 2016; 316:1298–1309 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
