

A pilot study on feasibility and hypothesis exploration: reducing on-scene length of stay of the emergency teams via ambulance dispatch teleconsultation for prehospital examination
- PMID: 40367011
- PMCID: PMC12094677
- DOI: 10.31744/einstein_journal/2025AO1469
A pilot study on feasibility and hypothesis exploration: reducing on-scene length of stay of the emergency teams via ambulance dispatch teleconsultation for prehospital examination
Abstract
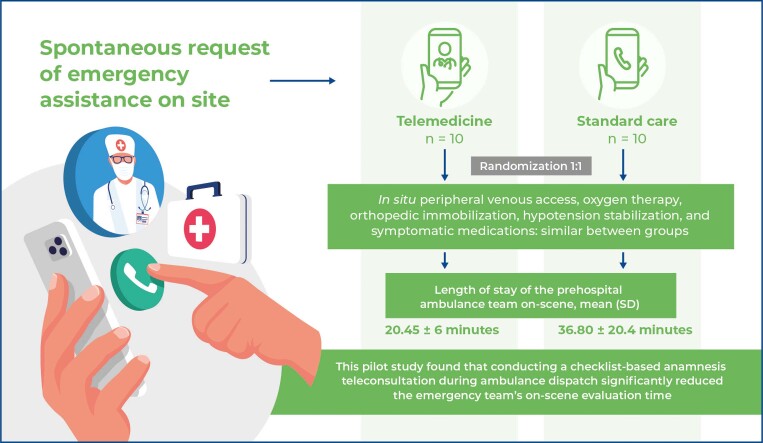
Background: This pilot study showed that teleconsultation during ambulance dispatch considerably reduced the emergency team's on-scene evaluation time, underscoring the potential of telemedicine in prehospital care. ■ Teleconsultation reduced on-scene time from 36.8 to 20.6 min (p=0.019). ■ Video-based prearrival anamnesis improved team efficiency. ■ Interventions and clinical profiles were similar across the groups. ■ Study supports broader telemedicine adoption in emergency care.
Objective: Ambulance transport time is an important metric in prehospital care. Limited studies have explored strategies to decrease on-scene time. We examined the effect of collecting telemedicine-based medical data during ambulance dispatch on the on-scene evaluation time of the prehospital team.
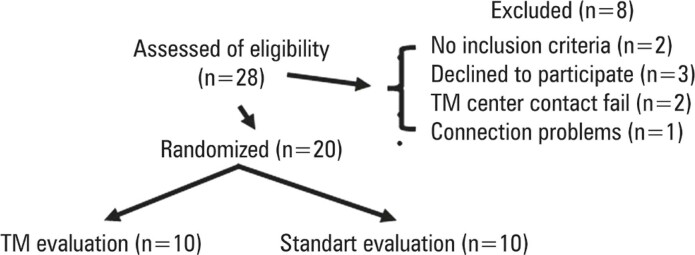
Methods: This randomized, single-center, open-label study included individuals aged >18 years who independently sought hospital emergency services and requested on-site emergency care. Individuals with primary trauma emergencies occurring outside the home, cardiac arrest cases, and situations in which video communication was unfeasible were excluded.
Results: Twenty patients were randomized to receive telemedicine assessment during ambulance dispatch or standard care with physician phone support. Both groups were comparable in age (53.2 ± 26.1 versus 63.4 ± 24.2 years, p=0.380), sex (50% versus 70% female, p=0.360), initial vital signs, and medical history. The main reasons for patients calls were falls from standing height (30%), followed by cardiovascular symptoms (20%), and acute neurological events (15%). Teleconsultation via a mobile application was successfully conducted in all cases. Furthermore, in situ interventions, including venous access, oxygen therapy, orthopedic immobilization, hypotension stabilization, and symptomatic treatment, were similar between the groups. The Telemedicine Group demonstrated a significantly shorter on-scene evaluation time (20.45 ± 6 min) than the Standard Group (36.80 ± 20.4 min, p = 0.019).
Conclusion: Conducting checklist-based anamnesis teleconsultation during ambulance dispatch considerably decreased the on-scene evaluation time of the emergency team. Further research with larger cohorts and different settings is required to better examine telemedicine's potential in this context.
Conflict of interest statement
Figures
References
-
- Turner J, Siriwardena AN, Coster J, Jacques R, Irving A, Crum A, et al. Developing new ways of measuring the quality and impact of ambulance service care: the PhOEBE mixed-methods research programme. Southampton (UK): NIHR Journals Library; 2019. Review. - PubMed
-
- O'Cathain A, Knowles E, Bishop-Edwards L, Coster J, Crum A, Jacques R, et al. Understanding variation in ambulance service non-conveyance rates: a mixed methods study. Southampton, UK: NIHR Journals Library; 2018. - PubMed
-
- Lincoln EW, Reed-Schrader E, Jarvis JL. StatPearls. Treasure Island (FL): StatPearls Publishing; 2020. EMS, Quality Improvement Programs. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
