

Universal health care delivery mitigates socioeconomic-related risk for adverse outcomes in hospitalised patients: Lessons from the COVID-19 pandemic in Australia
- PMID: 40367045
- PMCID: PMC12077700
- DOI: 10.1371/journal.pone.0322780
Universal health care delivery mitigates socioeconomic-related risk for adverse outcomes in hospitalised patients: Lessons from the COVID-19 pandemic in Australia
Abstract
Background: Internationally, socioeconomic disadvantage is related to severe outcomes of COVID-19. We investigated the impact of socioeconomic disadvantage on infection rates, hospitalisation, and in-hospital outcomes for COVID-19 with standardised medical care.
Methods: This retrospective cross-sectional study included SARS-CoV-2 PCR-confirmed patients ≥18 years, admitted to a major public hospital between January 2020 and December 2021. Severe COVID-19 outcomes were defined by a composite outcome of in-hospital death or other critical complications. A generalised linear regression model of demographic features, co-existing conditions, and socioeconomic status was used to determine the risks of the composite outcome.
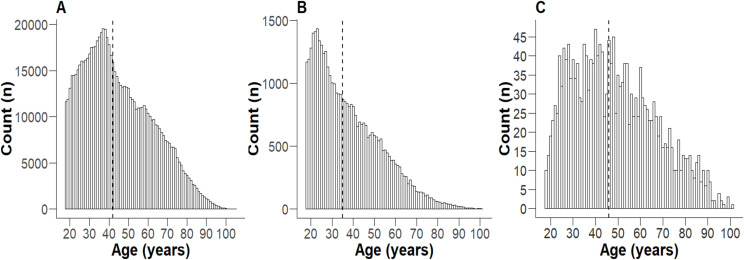
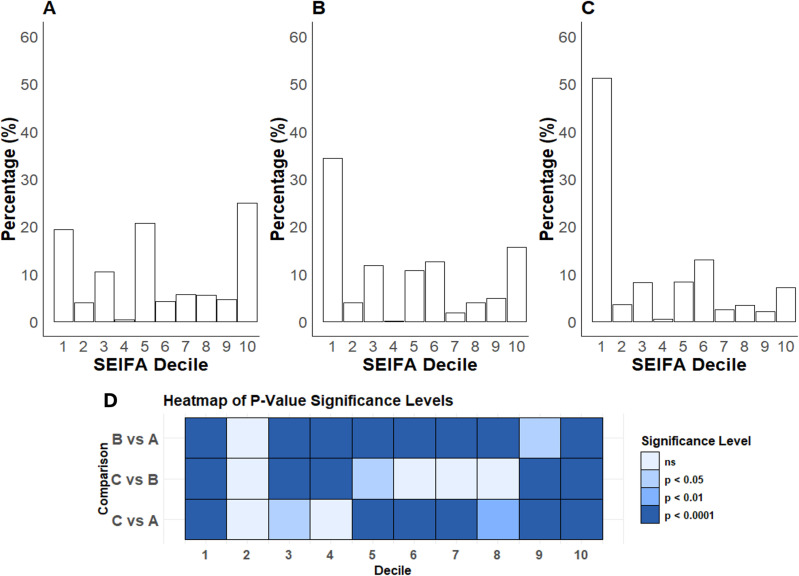
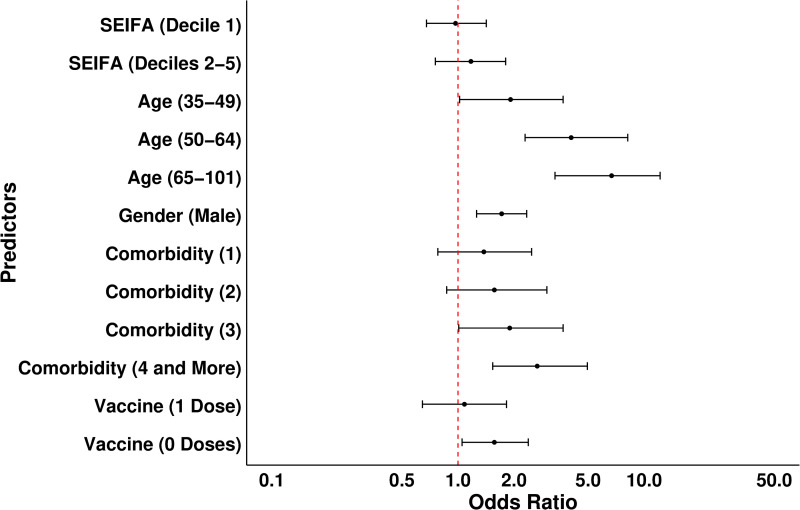
Results: Of 797,343 individuals ≥18 years in the health district, 50,906 (6.4%) were PCR-positive, and 1,962 were hospitalised. Compared with the whole health district population, infected individuals were younger (median [interquartile range] age 35 [25-48] years vs 42 [31-58] years) and from areas with the greatest socioeconomic disadvantage (34.4% vs 20%; both p < 0.0001). Hospitalised patients were older, with more females compared to the PCR-positive group (46 years [33-61], 53.5%, respectively; p < 0.001), and 51.2% were from postcodes with greatest socioeconomic disadvantage (p < 0.0001). The composite outcome occurred in 11.5%, with an in-hospital mortality of 3.8%. Higher risk of the composite outcome was observed in males (OR 1.72, 95% CI [1.26-2.42], p < 0.001), patients aged ≥ 65 years (OR 6.96, [3.3-14.6], p < 0.001), those with ≥ 4 comorbidities (OR 2.67, [1.54-4.63], p < 0.001), and unvaccinated patients (OR 1.57, [1.05-2.38], p < 0.05). The risk of composite outcome did not increase with socioeconomic disadvantage (OR 0.97, [0.68, 1.42], p = 0.64).
Conclusion: In the absence of capacity restraints, socioeconomic disadvantage was not associated with severe in-hospital outcomes in a well-resourced care environment despite increased rates of infection and hospitalisation. This highlights the impact of universally accessible, standardised, protocolised, high-quality in-hospital care in reducing the risk of adverse in-hospital outcomes in socioeconomically disadvantaged patients.
Copyright: © 2025 Faqihi et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The Impact of Socioeconomic Status on the Clinical Outcomes of COVID-19; a Retrospective Cohort Study.J Community Health. 2021 Aug;46(4):794-802. doi: 10.1007/s10900-020-00944-3. Epub 2021 Jan 2. J Community Health. 2021. PMID: 33387149 Free PMC article.
-
Characteristics and outcomes of people living with HIV hospitalised at tertiary healthcare institutions during the COVID-19 pandemic in Mexico City.BMC Infect Dis. 2024 May 24;24(1):524. doi: 10.1186/s12879-024-09208-0. BMC Infect Dis. 2024. PMID: 38789972 Free PMC article.
-
Sociodemographic factors associated with COVID-19 in-hospital mortality in Brazil.Public Health. 2021 Mar;192:15-20. doi: 10.1016/j.puhe.2021.01.005. Epub 2021 Jan 15. Public Health. 2021. PMID: 33607516 Free PMC article.
-
Incidence and mortality due to thromboembolic events during the COVID-19 pandemic: Multi-sourced population-based health records cohort study.Thromb Res. 2021 Jun;202:17-23. doi: 10.1016/j.thromres.2021.03.006. Epub 2021 Mar 8. Thromb Res. 2021. PMID: 33711754 Free PMC article.
-
Ethnic minority status as social determinant for COVID-19 infection, hospitalisation, severity, ICU admission and deaths in the early phase of the pandemic: a meta-analysis.BMJ Glob Health. 2021 Nov;6(11):e007433. doi: 10.1136/bmjgh-2021-007433. BMJ Glob Health. 2021. PMID: 34740916 Free PMC article.
References
-
- Department of Health and Human Services. Healthy People 2030, U.S. [Internet]. Washington (DC): U.S. Department of Health and Human Services; 2024. [cited 2024 Aug 12]. Available from: https://health.gov/healthypeople/objectives-and-data/social-determinants...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
