

ASSESSMENT OF EARLY INDICATORS FOR SEPSIS DEVELOPMENT IN MULTIPLE TRAUMA PATIENTS-THE SEPSIS AS TRAUMA OUTCOME PREDICTION (STOP) SCORE
- PMID: 40367515
- PMCID: PMC12278749
- DOI: 10.1097/SHK.0000000000002626
ASSESSMENT OF EARLY INDICATORS FOR SEPSIS DEVELOPMENT IN MULTIPLE TRAUMA PATIENTS-THE SEPSIS AS TRAUMA OUTCOME PREDICTION (STOP) SCORE
Abstract
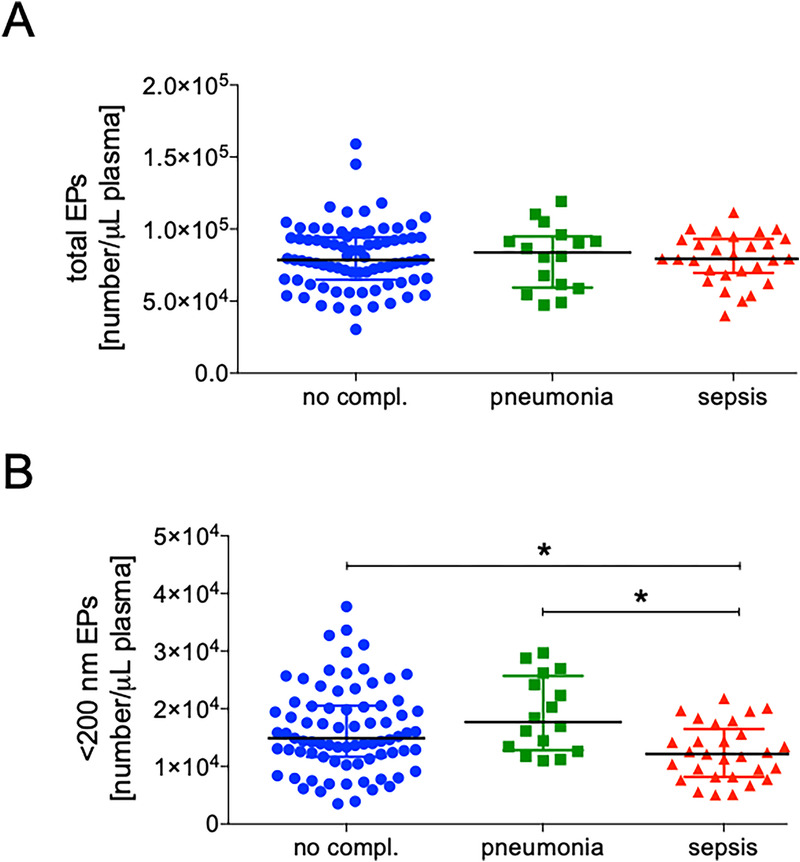
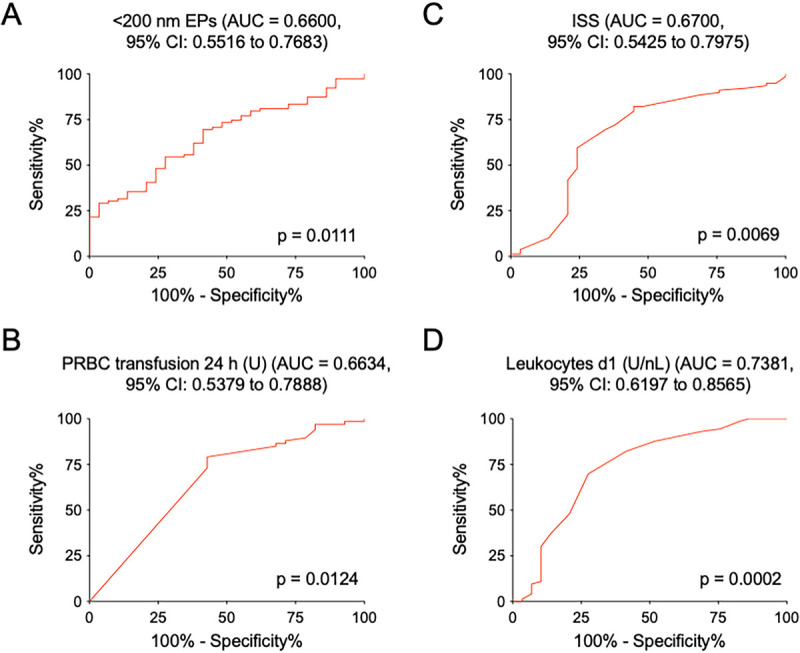
Background: Infections are common complications in critical care, particularly in patients with severe multiple trauma, who are at elevated risk due to trauma-induced immunological changes. The heterogeneity of trauma patients complicates their initial assessment, yet timely recognition of patients at risk is crucial for guiding therapy and preventive measures. This study evaluated risk factors for sepsis and pneumonia in multiple trauma patients, incorporating a novel parameter: cell-derived extracellular particles (EPs) in plasma. Methods: Severely injured multiple trauma patients aged 18-80 years with an Injury Severity Score (ISS) ≥16 were included. Patient- and injury-related parameters were assessed at the injury site, admission and during clinical course. EP counts in plasma were measured at admission using intravesicular staining. Key variables from the first 24 h were analyzed to develop an early risk assessment score. Results: Among 124 patients, 16 developed pneumonia, and 29 developed sepsis. Pneumonia was associated with significantly lower Glasgow Coma Scale scores, higher intubation rates at the injury site and elevated Sequential Organ Failure Assessment scores at admission. Sepsis correlated with higher ISS, increased 24-h transfusion rates, lower leukocyte counts on day 1, and decreased levels of small EPs in plasma at admission. These variables formed the weighted Sepsis as Trauma Outcome Prediction (STOP) score. A STOP score >3 had a positive predictive value of 59.4% within 24 h upon admission to the emergency department for subsequent sepsis development. Conclusion: The risk of pneumonia in severely injured trauma patients was linked to impaired consciousness and preexisting organ-dysfunctions at admission. High-risk sepsis patients could be identified on day 1 following trauma using the STOP score, which incorporates ISS, 24-h transfusion rates, leukocyte counts at day 1, and small EP rates at admission. This novel scoring system could facilitate targeted therapeutic and preventive strategies for distinguishing high-risk populations.
Keywords: AIS—Abbreviated Injury Scale; APACHE—Acute Physiology and Chronic Health Evaluation; ATLS—advanced trauma life support; AUC—area under the ROC curve; CI—confidence intervals; CRP—c-reactive protein; CT—computed tomography; DAMP—damage-associated molecular patterns; ED—emergency department; EP—extracellular particle; EV—extracellular vesicles; Extracellular particles; FFP—fresh frozen plasma; Fig—figure; ICU—intensive care unit; IL—interleukin; INR—international normalized ratio; IQR—interquartile range; ISS—Injury Severity Score; MISEV—minimal information for the study of extracellular vesicles; MODS—multiorgan dysfunction syndrome; PCT—procalcitonin; PPV—positive predictive value; PRBC—packed-red blood cell; ROC—receiver operating characteristic; SBP—systolic blood pressure; SEM—standard error of the mean; SIRS—systemic inflammatory response syndrome; SOFA—sequential organ failure assessment; STOP—sepsis as trauma outcome prediction; STROBE—Strengthening the Reporting of Observational Studies in Epidemiology; TPT—thromboplastin time; TSS—traumatic sepsis score; Tab—table; U—units; inflammation; polytrauma; prediction; risk assessment; scoring; vesicles.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Shock Society.
Conflict of interest statement
The authors report no conflicts of interest.
Figures

References
-
- Kollef MH Torres A Shorr AF, et al. Nosocomial infection. Crit Care Med. 2021;49(2):169–187. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
