

Unraveling mutagenic processes influencing the tumor mutational patterns of individuals with constitutional mismatch repair deficiency
- PMID: 40368937
- PMCID: PMC12078508
- DOI: 10.1038/s41467-025-59775-2
Unraveling mutagenic processes influencing the tumor mutational patterns of individuals with constitutional mismatch repair deficiency
Abstract
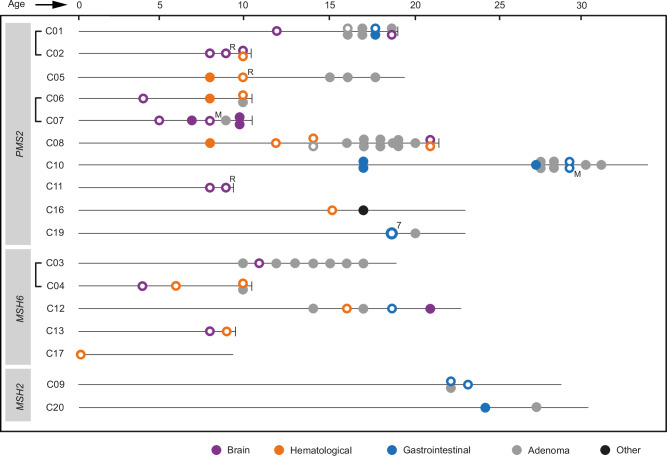
Constitutional mismatch repair deficiency (CMMRD), caused by bi-allelic germline variants in mismatch repair (MMR) genes, is associated with high cancer incidence early in life. A better understanding of mutational processes driving sequential CMMRD tumors can advance optimal treatment. Here, we describe a genomic characterization on a representative collection of CMMRD-associated tumors consisting of 41 tumors from 17 individuals. Mutational patterns in these tumors appear to be influenced by multiple factors, including the affected MMR gene and tumor type. Somatic polymerase proofreading mutations, commonly present in brain tumors, are also found in a T-cell lymphoblastic lymphoma displaying associated mutational patterns. We show prominent mutational patterns in two second primary hematological malignancies after temozolomide treatment. Furthermore, an indel signature, characterized by one-base pair cytosine insertions in cytosine homopolymers, is found in 54% of tumors. In conclusion, analysis of sequential CMMRD tumors reveals diverse mutational patterns influenced by the affected MMR gene, tumor type and treatment history.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures




References
-
- Sanders, M. A., et al. Life without mismatch repair. bioRxiv, 2021.2004.2014.437578, 10.1101/2021.04.14.437578 (2021).
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
