

Impact of the Triglyceride-Glucose index on all-cause and cardiovascular mortalities across different metabolic health and obesity statuses in US adults
- PMID: 40369462
- PMCID: PMC12077056
- DOI: 10.1186/s12889-025-22901-2
Impact of the Triglyceride-Glucose index on all-cause and cardiovascular mortalities across different metabolic health and obesity statuses in US adults
Abstract
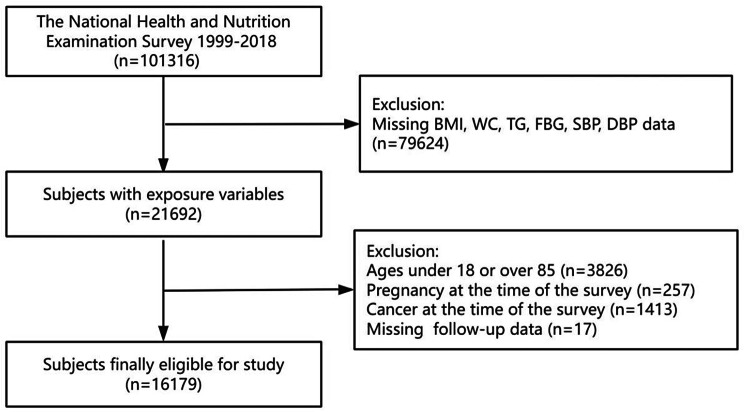
Background: Data for the study cohort were sourced from the National Health and Nutrition Examination Survey (1999-2018). Study participants were classified as obese (BMI ≥ 30 kg/m²) or nonobese (BMI < 30 kg/m²) then further categorized as metabolically healthy or unhealthy on the basis of metabolic syndrome criteria, resulting in four groups: metabolically healthy obese (MHO), metabolically unhealthy obese (MUO), metabolically healthy nonobese (MHNO), and metabolically unhealthy nonobese (MUNO). Complex sampling statistical methods were employed for descriptive analysis. The associations between the TyG index and mortality, including all-cause and cardiovascular mortalities, were examined by using multivariable Cox regression and restricted cubic splines (RCS). The reliability of the results was confirmed through multiple sensitivity analyses.
Methods: Data for the study cohort were sourced from the National Health and Nutrition Examination Survey (1999-2018). Study participants were classified as obese (BMI ≥ 30 kg/m²) or nonobese (BMI < 30 kg/m²) then further categorized as metabolically healthy or unhealthy on the basis of metabolic syndrome criteria, resulting in four groups: metabolically healthy obese (MHO), metabolically unhealthy obese (MUO), metabolically healthy nonobese (MHNO), and metabolically unhealthy nonobese (MUNO). Complex sampling statistical methods were employed for descriptive analysis. The associations between the TyG index and mortality, including all-cause and cardiovascular mortalities, were examined by using multivariable Cox regression and restricted cubic splines (RCS). The reliability of the results was confirmed through multiple sensitivity analyses.
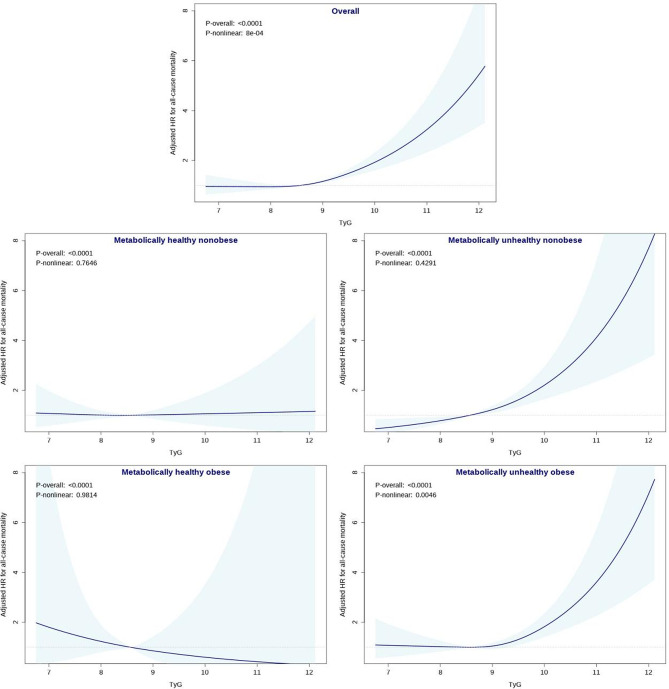
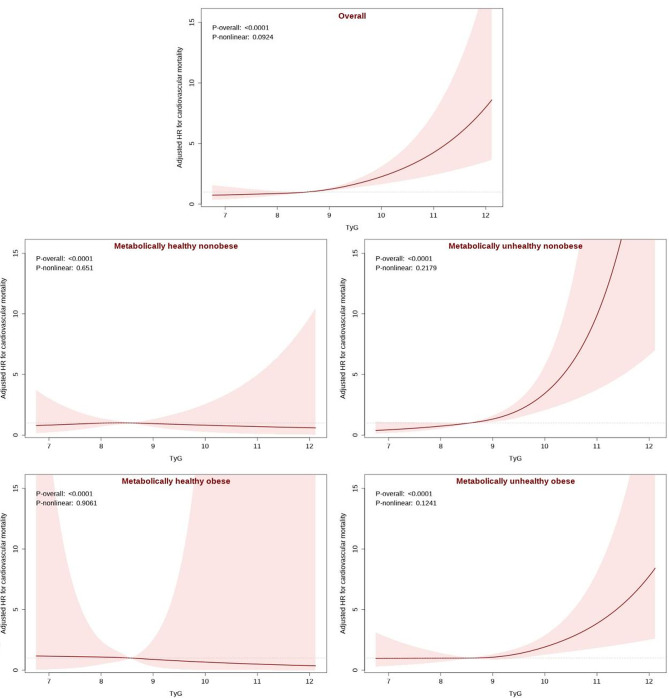
Results: A total of 16 179 participants were included, with a median follow-up of 129 months. Over this follow-up period, 1875 participants (11.59%) died from all causes, including 568 (3.51%) who died due to cardiovascular diseases. After adjustment for confounding variables, the TyG index significantly predicted mortality in the overall and metabolically unhealthy populations: for each one standard deviation increase in the TyG index, all-cause mortality increased by 1.42 times (95% confidence interval [CI]: 1.27, 1.58) in the overall population, by 1.62 times (95% CI: 1.36, 1.93) in the MUNO group, and by 1.47 times (95% CI: 1.26, 1.71) in the MUO group. Cardiovascular mortality in the overall population increased by 1.52 times (95% CI: 1.27, 1.82), that in the MUNO group increased by 2.01 times (95% CI: 1.49, 2.72), and that in the MUO group increased by 1.47 times (95% CI: 1.14, 1.88). No significant association was found in the metabolically healthy populations regardless of obesity status. RCS and sensitivity analyses further confirmed and visualized these conclusions.
Conclusions: The TyG index is positively correlated with mortality risk in the overall and metabolically unhealthy populations but not in the metabolically healthy populations. This finding indicates that the predictive value of the TyG index for mortality differs across populations, highlighting the necessity of accounting for metabolic status when the TyG index is used for prognostic evaluation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The studies involving humans were approved by the US Centers for Disease Control and Prevention. The studies were conducted in accordance with local legislation and institutional requirements. The participants provided written informed consent to participate in this study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
The Association between Cardio-metabolic and hepatic indices and anthropometric measures with metabolically obesity phenotypes: a cross-sectional study from the Hoveyzeh Cohort Study.BMC Endocr Disord. 2023 May 29;23(1):122. doi: 10.1186/s12902-023-01372-9. BMC Endocr Disord. 2023. PMID: 37246210 Free PMC article.
-
Triglyceride-Glucose Index Predicts Cardiovascular Outcome in Metabolically Unhealthy Obese Population: A Nationwide Population-Based Cohort Study.J Obes Metab Syndr. 2022 Jun 30;31(2):178-186. doi: 10.7570/jomes21086. Epub 2022 Jun 13. J Obes Metab Syndr. 2022. PMID: 35691685 Free PMC article.
-
Obesity measures, metabolic health and their association with 15-year all-cause and cardiovascular mortality in the SAMINOR 1 Survey: a population-based cohort study.BMC Cardiovasc Disord. 2021 Oct 21;21(1):510. doi: 10.1186/s12872-021-02288-9. BMC Cardiovasc Disord. 2021. PMID: 34674643 Free PMC article.
-
Differences in the levels of inflammatory markers between metabolically healthy obese and other obesity phenotypes in adults: A systematic review and meta-analysis.Nutr Metab Cardiovasc Dis. 2024 Feb;34(2):251-269. doi: 10.1016/j.numecd.2023.09.002. Epub 2023 Sep 9. Nutr Metab Cardiovasc Dis. 2024. PMID: 37968171
-
Metabolically healthy obesity and risk of incident type 2 diabetes: a meta-analysis of prospective cohort studies.Obes Rev. 2014 Jun;15(6):504-15. doi: 10.1111/obr.12157. Epub 2014 Mar 24. Obes Rev. 2014. PMID: 24661566 Free PMC article. Review.
Cited by
-
Triglyceride glucose-weight-adjusted waist index as a cardiovascular mortality predictor: incremental value beyond the establishment of TyG-related indices.Cardiovasc Diabetol. 2025 Jul 30;24(1):306. doi: 10.1186/s12933-025-02873-8. Cardiovasc Diabetol. 2025. PMID: 40739633 Free PMC article.
References
-
- World Obesity Federation. Obesity Atlas 2024 [Internet]. 2024. Available from: https://data.worldobesity.org/publications/?cat=22
-
- Gilden AH, Catenacci VA, Taormina JM, Obesity. Ann Intern Med. 2024;177:ITC65–80. - PubMed
-
- Stefan N, Häring H-U, Hu FB, Schulze MB. Metabolically healthy obesity: epidemiology, mechanisms, and clinical implications. Lancet Diabetes Endocrinol. 2013;1:152–62. - PubMed
-
- Stefan N, Schulze MB. Metabolic health and cardiometabolic risk clusters: implications for prediction, prevention, and treatment. Lancet Diabetes Endocrinol. 2023;11:426–40. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
