

Differences in timeliness, completeness and drop-out rates of MMRV and DTP containing vaccines among Ultra-Orthodox Jews and others in a deprived Northern Israel city: an ecological study
- PMID: 40369540
- PMCID: PMC12080259
- DOI: 10.1186/s12939-025-02504-4
Differences in timeliness, completeness and drop-out rates of MMRV and DTP containing vaccines among Ultra-Orthodox Jews and others in a deprived Northern Israel city: an ecological study
Abstract
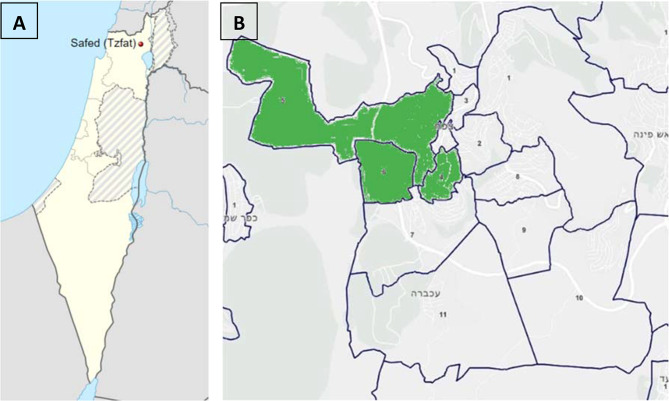
Background: The Ultra-Orthodox Jewish (UO) population has been affected by pertussis, polio, and measles outbreaks. Safed, a deprived, undervaccinated city in Israel's North, has a large UO population concentrated in specific neighborhoods. We determined whether in Safed UO population concentration was associated with DTP- containing and MMRV1 vaccines coverage, timeliness and drop-out rates.
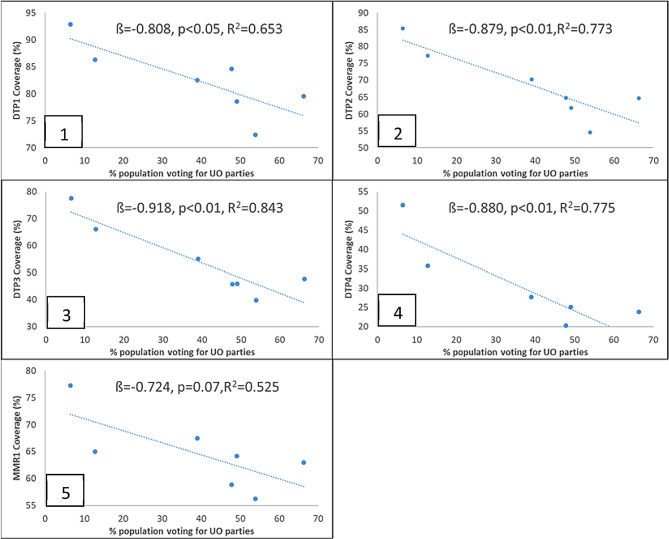
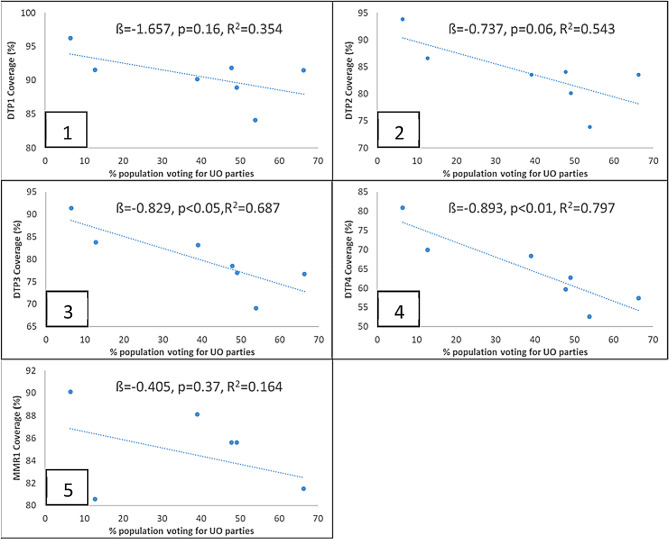
Method: For each of Safed's statistical areas, we estimated UO population based on the proportion of votes for UO political parties in Israel's 2020 general elections. We determined whether this proportion was associated with timely and delayed MMRV1 and DTP vaccine coverage for children born 2017-2022 using simple linear regression. We compared DTP and MMRV1 coverage and drop-out rates in UO areas (> 50% vote for UO parties) to others, using chi-square tests.
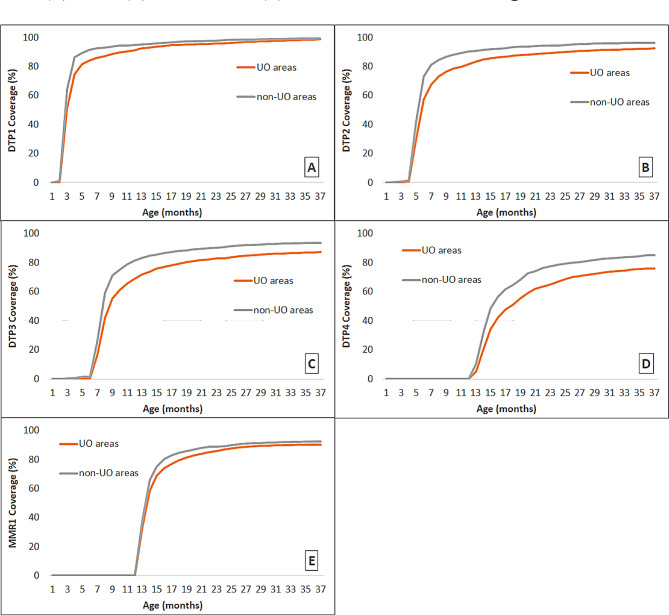
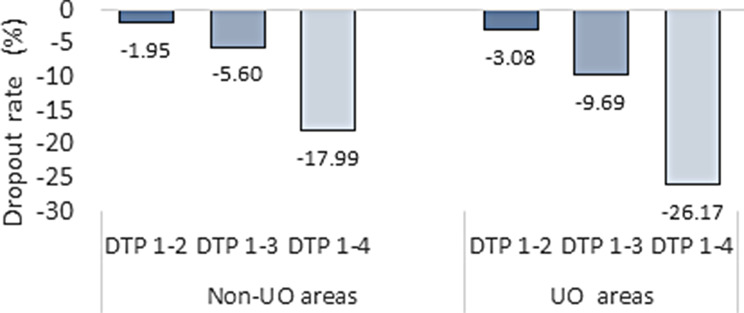
Results: All eligible 4385 children residing in Safed were included in the MMRV1 and DTP analyses. Vaccine coverage was significantly lower in UO areas compared to non-UO for all doses of DTP and MMRV1 at expected age (-11.8, -15.8, -16.6, -11.8 and - 7.1% points (pp) respectively, P < 0.005) - and at 36 months old (-0.5, -3.9, -6.2, -9.3 and - 2% points respectively, P < 0.005). Gaps narrowed more for MMRV1 (from 7.1 to2 pp), than for DTP4 (from 11.8 to9.3 pp). Increasing UO vote was associated with decreased timely coverage for DTP but not MMRV. DTP1-4 drop-out rates were larger in the UO areas than in non-UO areas (26.2% vs. 18%).
Conclusions: Vaccine coverage was lower in UO neighborhoods, even in a peripheral city where coverage in non-UO areas is already low. Coverage differences between UO and non-UO populations decreased with time for MMRV1 but not DTP. Our findings suggest timeliness should be considered alongside non-vaccination, and vaccination behavior may be vaccine-specific in the UO population.
Keywords: DTP; Equity; Israel; Jewish; MMRV; Religion; Vaccine coverage.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Ethics Committee of the Bar Ilan University, Faculty of Medicine, approved the study, approval number: 11-2021. We also received approval from the Helsinki Committee of the Ministry of Health in Israel for accessing the data, approval number: MOH-076-2022. The data is based on the anonymized vaccine registry obtained from the Ministry of Health, and individual consent is not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- World Health Organization. Measles vaccines: WHO position paper– April 2017. Wkly Epidemiol Rec. 2017;92:205–27.
-
- NHS, Childhood Vaccination C, Statistics E. 2023-24 [Internet]. NHS. 2024. https://digital.nhs.uk/data-and-information/publications/statistical/nhs.... Accessed 22 January 2025.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
