

ESR1 testing on FFPE samples from metastatic lesions in HR + /HER2- breast cancer after progression on CDK4/6 inhibitor therapy
- PMID: 40369610
- PMCID: PMC12079830
- DOI: 10.1186/s13058-025-02020-x
ESR1 testing on FFPE samples from metastatic lesions in HR + /HER2- breast cancer after progression on CDK4/6 inhibitor therapy
Abstract
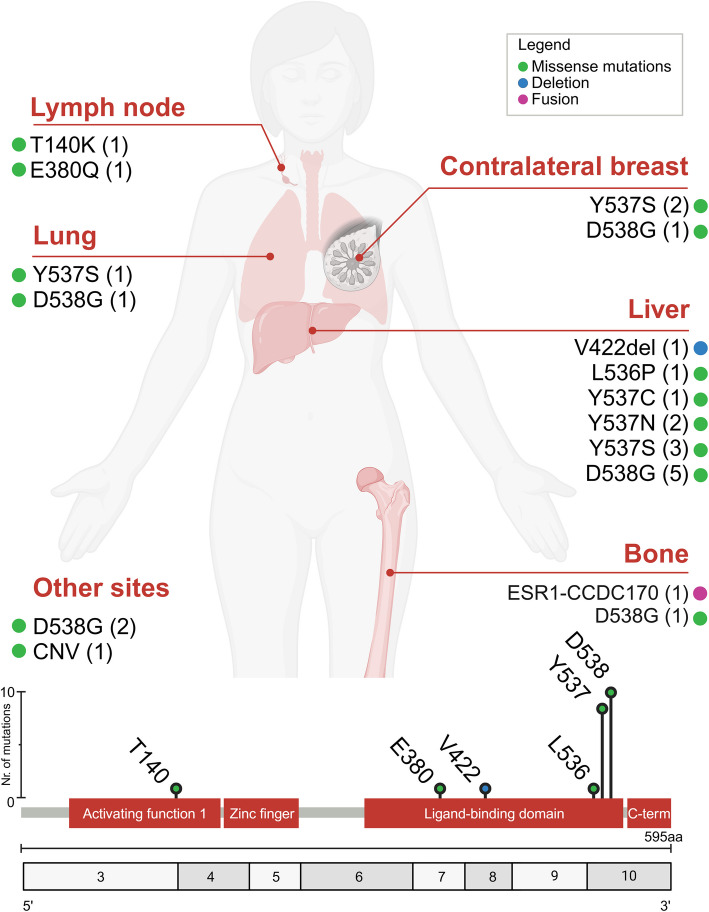
Mutations in ESR1 play a critical role in resistance to endocrine therapy (ET) in hormone receptor-positive (HR +)/HER2- metastatic breast cancer (MBC). Testing for ESR1 mutations is essential for guiding treatment with novel oral selective estrogen receptor degraders (SERDs) like elacestrant or camizestrant. While most studies have utilized liquid biopsy (LB) for mutation detection, the role of formalin-fixed paraffin-embedded (FFPE) tissue biopsy in this context remains unclear. In this study, we analyzed a cohort of HR + /HER2- MBC patients who experienced resistance to ET and CDK4/6 inhibitors. Next-generation sequencing (NGS) was performed on FFPE biopsy samples obtained from metastatic sites at the time of disease progression. ESR1 mutations were detected in 24 out of 38 patients (63.2%), with p.D538G identified in 10 patients (45.5%) and p.Y537S in 6 patients (27.2%) as the most frequent alterations. One patient exhibited dual ESR1 mutations, and a recurrent ESR1-CCDC170 gene fusion was identified, underscoring the diversity and potential interplay of genetic alterations driving resistance in HR + /HER2- MBC. Notably, lung metastases were significantly more common in ESR1 mutant cases (8/24, 33.3%) compared to wild-type cases (1/14, 7.1%), while liver metastases showed no difference between mutant (12/24, 50.0%) and wild-type groups (7/14, 50.0%). Co-mutations in actionable pathways, particularly PIK3CA, were observed in n = 10 ESR1 mutant tumors (41.6%), highlighting their contribution to resistance mechanisms and posing significant challenges for treatment selection, as these alterations may necessitate combination therapies to effectively target multiple resistance pathways. This study presents new insights into the prevalence and clinical significance of ESR1 mutations in HR + /HER2- MBC, highlighting the potential utility of FFPE biopsy samples as a viable alternative or complementary approach to LB for mutation detection, particularly in resource-limited settings where access to ctDNA analysis may be constrained.
Keywords: ESR1 mutations; CDK4/6 inhibitors; Endocrine therapy resistance; FFPE tissue biopsy; Metastatic breast cancer (MBC); SERDs; ctDNA.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki and received approval by the Institutional Review Board (IRB) of the European Institute of Oncology (IEO) IRCCS, Milan, Italy (approval #UID3472); in compliance with the EU General Data Protection Regulation (GDPR), all information regarding the recruited patients were pseudo-anonymized. Informed consent was obtained from all participants prior to their inclusion in the study. Competing interests: K.V. Has received honoraria for speaker bureau from Merck Sharp & Dohme (MSD), Roche, and AstraZeneca; G.Curs. from Veracyte; M.D-E from AstraZeneca, A.M. has received support from Menarini Group and served on the Speakers' Bureau for Roche and AstraZeneca. F.P. has received personal fees (as consultant and/or speaker bureau) from Menarini group and Roche. S.S. reported speaker fees from Novartis, Pfizer, Roche, Lilly, BMS, and MSD. Advisory role for AstraZeneca and Daiichi-Sankyo. C.D-A. reported grants from Daiichi Sankyo, Gilead, and Novartis; and personal fees from Pfizer, AstraZeneca, Eli Lilly, Novartis, and Roche outside the submitted work. G.T. reports personal fees (as speaker bureau or advisor) from Roche, MSD, Pfizer, Boehringer Ingelheim, Eli Lilly, BMS, GSK, Menarini, AstraZeneca, Amgen and Bayer, unrelated to the current work. U.M. has received personal fees (as consultant and/or speaker bureau) from Boehringer Ingelheim, Roche, MSD, Amgen, Thermo Fisher Scientific, Eli Lilly, Diaceutics, GSK, Merck and AstraZeneca, Janssen, Diatech, Novartis and Hedera unrelated to the current work. G.P. has received personal fees (as consultant and/or speaker bureau) from Boehringer Ingelheim, Roche, MSD, Amgen, Diaceutics, Merck, AstraZeneca, Novartis, Daiichi Sankyo, Exact Sciences, Sakura Finetek Europe B.V., Diatech Pharmacogenetics unrelated to the current work. A.B. has advisory and consulting roles for Roche, MSD, Novartis, Pfizer, Lilly, Amgen, BMS, Gilead, Sofos, Daichii, and AstraZeneca. G.V. reported personal fees from Roche, AstraZeneca, Daiichi Sankyo, Pfizer, Agilent, Eli Lilly, and Gilead. G.Curi. has received honoraria for speaker engagements from Roche, Seattle Genetics, Novartis, Lilly, Pfizer, Foundation Medicine, NanoString, Samsung, Celltrion, BMS, and MSD; honoraria for consultancy from Roche, Seattle Genetics, and NanoString; honoraria for participation in advisory boards from Roche, Lilly, Pfizer, Foundation Medicine, Samsung, Celltrion, and Mylan; honoraria for writing engagements from Novartis and BMS; and honoraria for participation in the Ellipsis Scientific Affairs Group. He has also received institutional research funding for conducting phase I and II clinical trials from Pfizer, Roche, Novartis, Sanofi, Celgene, Servier, Orion, AstraZeneca, Seattle Genetics, AbbVie, Tesaro, BMS, Merck Serono, Merck Sharp & Dohme, Janssen-Cilag, Philogen, Bayer, Medivation, and Medimmune. E.G-R. has received advisory fees, honoraria, travel accommodations/expenses, grants, and/or non-financial support from AstraZeneca, Exact Sciences, GSK, Illumina, MSD, Novartis, Roche, and Thermo Fisher Scientific. C.C. has participated in advisory or consultancy roles and speakers' bureau engagements for Eli Lilly, Pfizer, Novartis, Roche, AstraZeneca, MSD, Daiichi Sankyo, Gilead, and Seagen. N.F. has received honoraria for consulting, advisory role, speaker bureau, travel, and/or research grants from Merck Sharp & Dohme (MSD), Merck, Novartis, AstraZeneca, Roche, Menarini Group, Daiichi Sankyo, GlaxoSmithKline (GSK), Gilead, Sysmex, Genomic Health, Veracyte, Sakura, Leica Biosystems, Lilly, Pfizer, ThermoFisher, Abbvie. These companies had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and/or in the decision to publish the results. All other authors declare no potential conflicts of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
