

Treatment preferences among individuals with primary hyperoxaluria type 1 (PH1): a real-world study
- PMID: 40369613
- PMCID: PMC12080053
- DOI: 10.1186/s13023-025-03738-9
Treatment preferences among individuals with primary hyperoxaluria type 1 (PH1): a real-world study
Abstract
Background: Primary hyperoxaluria type 1 (PH1) is a rare genetic disorder causing excessive oxalate production, damaging kidneys and other organs. Nedosiran, launched in the U.S. for individuals with PH1 (≥ 9 years of age; estimated glomerular filtration rate [eGFR] ≥ 30 mL/min/1.73 m2), can be self- or caregiver-administered at home with fixed-dosing for patients ≥ 12 years of age. This real-world study aimed to understand treatment preferences among individuals with PH1, highlighting challenges in administration of current treatments.
Methods: A cross-sectional web-based survey was conducted among U.S.-based adults (aged ≥ 18) diagnosed with PH1. The survey consisted of a 20-25 min questionnaire and was conducted from October to December 2023.
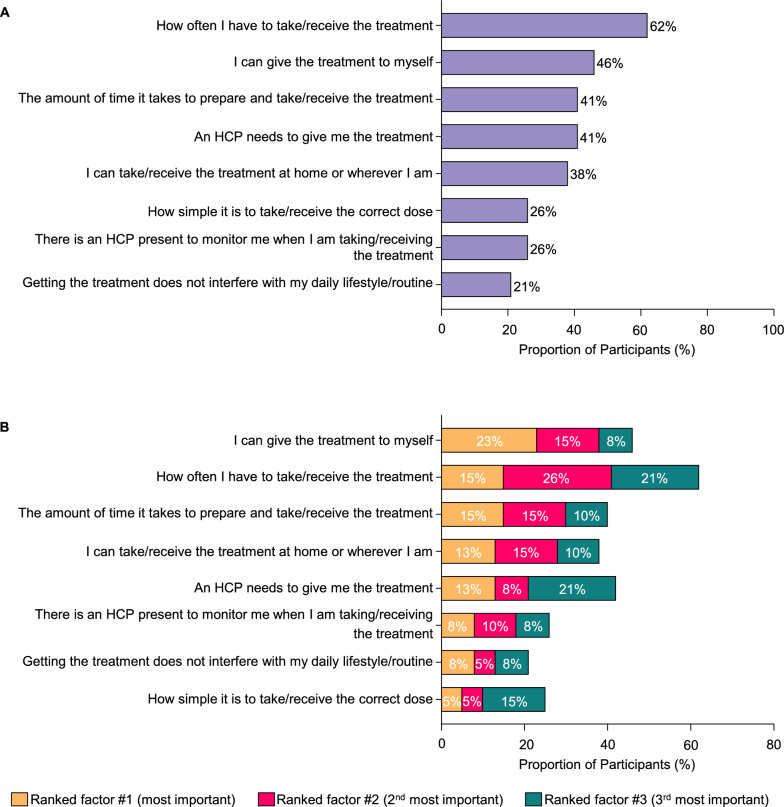
Results: The study participants (N = 39) included both male (N = 26) and female (N = 13) adults with PH1. Participants came from a range of community settings, including urban (46%), rural (39%), and suburban (15%); and were full- or part-time workers (56%) or students (41%). Most participants were on lumasiran therapy (95%) for an average of 1 year (range: 0.3-1.8 years). The survey revealed that the commonly reported factors important for treatment selection among participants living with PH1 were frequency of administration, treatment administrator, time required for treatment, and place of administration. The ability to self-administer was ranked as the top choice by most participants. Over half (56%) found quarterly injections easy or very easy. Similarly, 56-59% found home administration, whether self- or healthcare provider (HCP)-administered, easy or very easy. Nearly half (46%) considered injections at medical facilities challenging or very challenging. The majority indicated traveling > 15 min for injections would be burdensome (57%) and arranging appointments problematic (54%). When comparing administration methods, 72% preferred self-injection over HCP-administered injections. Regarding treatment regimens, 57% found it easy or very easy to receive monthly injections initially, before switching to quarterly. Additionally, 64% preferred a medication dosage that is not weight-based. While participants expressed a preference for less frequent treatments, 67% preferred self-injection at home over medical facility injections, and 67% preferred monthly injections at home over quarterly injections at a medical facility.
Conclusions: This study shows that patients with PH1 value treatments that are convenient and fit their lifestyle.
Keywords: Patient survey; Primary hyperoxaluria; Real-world study; Treatment preferences.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Before enrollment of patients into this study, the protocol, ICF, any promotional material/advertisements, and any other written information to be provided to participants have been reviewed and approved by the IRB (tracking number 20234228). Consent for publication: Not applicable. Competing interests: DSG is a consultant for Novo Nordisk, Alnylam, Arbor Biotechnologies, and Lilac Pharmaceuticals; Owner of Moonstone Nutrition Inc. FM is a consultant for Travere and Antares Pharma. JVC is an employee of Genesis Research Group, which received payment from Novo Nordisk Inc to oversee this research. RZ, BP, and MS are employees of Stratevi, LLC, which received payment from Novo Nordisk Inc to design, implement, and interpret findings from this research. SS is an employee of Novo Nordisk Inc.
Figures






References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
