

Dihydroartemisinin-piperaquine versus sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria in pregnancy: a systematic review and individual participant data meta-analysis
- PMID: 40370584
- PMCID: PMC12076784
- DOI: 10.1016/j.eclinm.2025.103202
Dihydroartemisinin-piperaquine versus sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria in pregnancy: a systematic review and individual participant data meta-analysis
Abstract
Background: High-grade Plasmodium falciparum resistance to sulfadoxine-pyrimethamine in east and southern Africa has prompted trials evaluating intermittent preventive treatment in pregnancy (IPTp) with dihydroartemisinin-piperaquine as an alternative to sulfadoxine-pyrimethamine. We aimed to provide an updated and comprehensive review of trials conducted in areas of high P. falciparum resistance that compared the efficacy of two types of IPTp regimens on maternal, birth, and infant outcomes.
Methods: We conducted two-stage, individual participant data meta-analyses of randomised trials comparing IPTp with dihydroartemisinin-piperaquine to sulfadoxine-pyrimethamine on maternal, birth, and infant outcomes. We searched the WHO International Clinical Trials Registry Platform, ClinicalTrials.Gov, PubMed, and the Malaria in Pregnancy Consortium Library, on July 30, 2020 (updated on September 24, 2024), without restrictions by publication date, peer-review status, or language. Eligible trials enrolled HIV-uninfected pregnant women, followed participants to delivery, included participants with no prior IPTp use during the current pregnancy, and were conducted in areas with high-level parasite resistance to sulfadoxine-pyrimethamine (i.e., PfDHPS 540E ≥ 90% and/or 581G>0%). Only singleton pregnancies were analysed. The primary endpoint was a composite measure of any adverse pregnancy outcome defined as fetal or neonatal loss, small-for-gestational age, low birthweight, or preterm birth. Summary estimates were generated using a random-effects model. Gravidity subgroup analyses were performed. Causal mediation analyses were used to investigate the maternal mechanisms underlying the effect of IPTp regimens on birth outcomes. The meta-analysis is registered in PROSPERO (CRD42020196127).
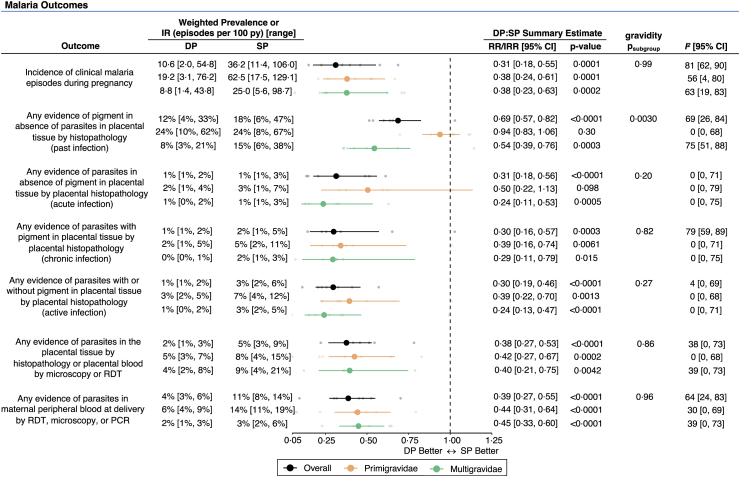
Findings: Of 85 screened records, six trials (one multi-country trial) from Kenya, Malawi, Uganda and Tanzania contributed data on 6646 pregnancies. Compared to sulfadoxine-pyrimethamine, dihydroarteminsinin-piperaquine was associated with a 69% [95% CI: 45%-82%] lower incidence of clinical malaria during pregnancy, a 62% [37%-77%] lower risk of placental parasitaemia, and a 17% [0%-31%] lower incidence of moderate maternal anaemia. In contrast, sulfadoxine-pyrimethamine was associated with higher mean maternal weight gain (34 g/week [17-51]). There were no statistically significant differences in the composite adverse pregnancy outcome (RR = 1.05 [0.92-1.19]; I 2 = 48%). Individual components of the primary outcome showed no statistically significant differences in the risks of fetal loss (RR = 0.94 [0.61-1.46]), preterm birth (RR = 0.93 [0.76-1.14]), low birthweight (RR = 1.09 [0.83-1.43]), or neonatal loss (RR = 0.73 [0.42-1.26]), though findings may have been underpowered. Small-for-gestational-age risk was 15% (3%-24%) lower in the sulfadoxine-pyrimethamine arm, particularly among multigravidae (a 22% reduction vs 9% in primigravidae). Among multigravidae, infant stunting and underweight by two months was 20% [8%-30%] and 35% [17%-49%] lower in the sulfadoxine-pyrimethamine arm compared to dihydroartemisinin-piperaquine. Compared to dihydroartemisinin-piperaquine, sulfadoxine-pyrimethamine was associated with higher mean newborn birthweight (mean difference (MD) = 50 g [95% CI: 13-88]; p = 0.0090, I2 = 61%) and BWGA z-scores (MD = 0.12 [95% CI: 0.05-0.20]; p = 0.0012, I2 = 51%), but not gestational age at birth (MD = 0 weeks [95% CI: -0.11 to 0.12]; p = 0.94; I2 = 42%). Infant wasting by two months was 13% [3%-22%] lower in the sulfadoxine-pyrimethamine arm, regardless of gravidity. Mediation analyses indicated that 15% [0%-19%] of sulfadoxine-pyrimethamine's superior effect on small-for-gestational-age risk was mediated by its greater impact on gestational weight gain.
Interpretation: In areas with high P. falciparum sulfadoxine-pyrimethamine resistance, dihydroartemisinin-piperaquine offers superior antimalarial efficacy than sulfadoxine-pyrimethamine. However, replacing sulfadoxine-pyrimethamine with dihydroartemisinin-piperaquine alone may not lead to improved maternal and infant health outcomes. Instead, it could result in slightly reduced gestational weight gain and a modest increase in the risk of small-for-gestational age births, and poor infant growth by two months of age. Future research evaluating alternative strategies for IPTp are needed.
Funding: This work was supported by the Bill and Melinda Gates Foundation and Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Keywords: Antimalarial resistance; Dihydroartemisinin-piperaquine; Intermittent preventive treatment in pregnancy; Non-malarial effects; Plasmodium falciparum; Sulfadoxine-pyrimethamine.
© 2025 The Author(s).
Conflict of interest statement
JRG has served as the co-Chair of the Roll Back Malaria, Malaria in Pregnancy Working Group and as a member of the Data Safety Monitoring Boards for the PYRAPREG and ASPIRE trials; no compensation was received. JH and FOtK reports funding from EDCTP2 supported by the European Union (grant number TRIA-2015-1076-IMPROVE), and the MRC/DFID/Wellcome Trust's Joint Global Health Trials scheme, and the Swedish International Development Cooperation Agency. All other authors declare no competing interests.
Figures




Update of
-
Dihydroartemisinin-piperaquine versus sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria in pregnancy: a systematic review and individual participant data meta-analysis.medRxiv [Preprint]. 2024 Nov 26:2024.11.23.24315401. doi: 10.1101/2024.11.23.24315401. medRxiv. 2024. Update in: EClinicalMedicine. 2025 Apr 29;83:103202. doi: 10.1016/j.eclinm.2025.103202. PMID: 39649586 Free PMC article. Updated. Preprint.
References
-
- Desai M., Ter Kuile F.O., Nosten F., et al. Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis. 2007;7(2):93–104. - PubMed
-
- World Health Organization . World Health Organization; Geneva, Switzerland: 2024. World malaria report 2023.
-
- World Health Organization . World Health Organization; 2022. WHO guidelines for malaria, 3 June 2022.
Grants and funding
LinkOut - more resources
Full Text Sources
