

Primary Cutaneous CD4+ Small/Medium T-cell Lymphoproliferative Disorder in a Young Japanese Male Patient
- PMID: 40370866
- PMCID: PMC12075897
- DOI: 10.7759/cureus.82211
Primary Cutaneous CD4+ Small/Medium T-cell Lymphoproliferative Disorder in a Young Japanese Male Patient
Abstract
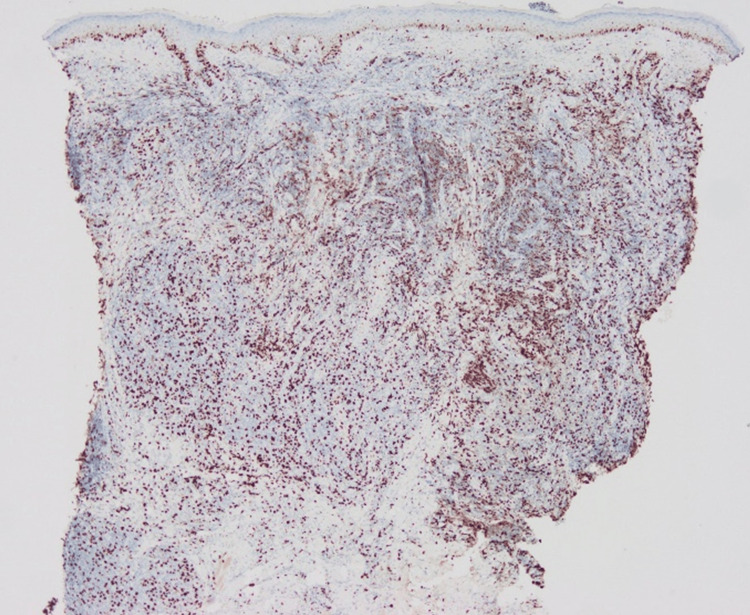
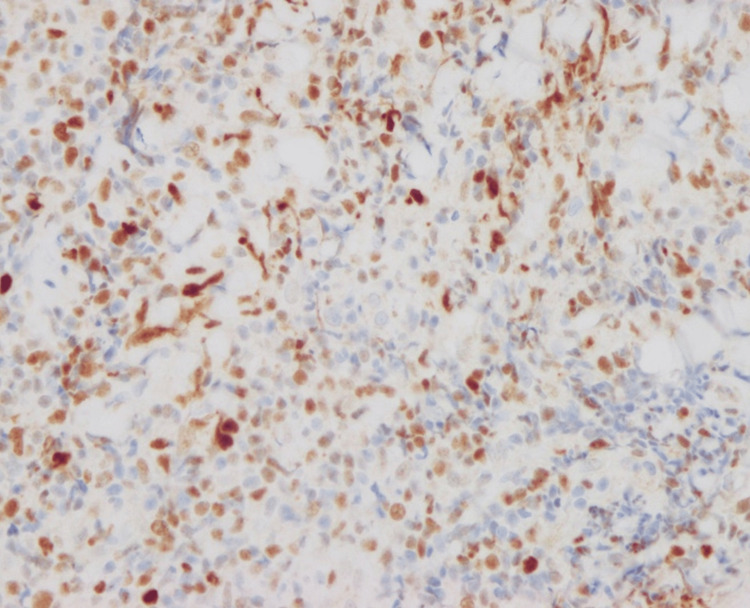
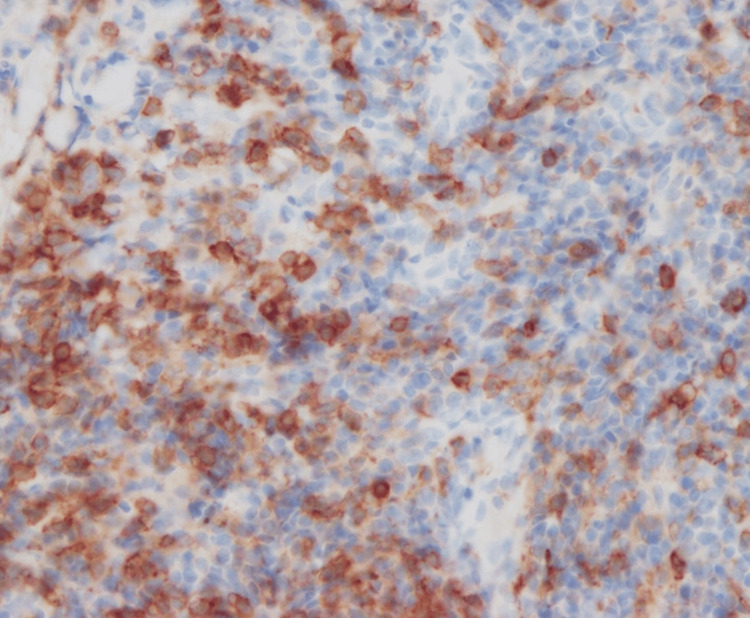
A 34-year-old man became aware of an erythematous nodule on the left nasal wing. He was treated with topical steroids and oral antibacterial agents at his local doctor, but his condition did not improve, and he was referred to our hospital. A skin biopsy revealed diffuse cellular infiltration through the dermis. No epidermotropism was seen. The major infiltrate was small to medium-sized lymphoid cells. The number of CD3+ cells was almost the same as that of CD20+ cells, while CD4+ cells were dominant over CD8+ cells. Atypical lymphocytes were positive for BCL6 and PD-1. Polymerase chain reaction (PCR) analysis of immunoglobulin heavy chain and T-cell receptor gene rearrangements on paraffin-embedded tissue sections revealed a clonal expansion of T-cells. The patient was diagnosed as having primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder (PCSM-LPD) and treated with fludroxycortide tape. The red nodule completely disappeared after three months. Nuclear staining for nuclear factor of activated T-cells c1 (NFATc1), which had been suggested to be useful in distinguishing PCSM-LPD from pseudolymphoma, was negative in our case. Our case was considered to be typical of PCSM-LPD among existing reports of PCSM-LPD from Japan, except for the young age of the patient. Our case suggested that young cases with PCSM-LPD may have been misdiagnosed with cutaneous pseudolymphoma (CPL), which may be one of the reasons why this type of lymphoproliferative disorder has been reported to occur in elderly people.
Keywords: bcl6; cutaneous pseudolymphoma; nuclear staining for nuclear factor of activated t-cells c1 (nfatc1); primary cutaneous cd4+ small/medium t-cell lymphoproliferative disorder (pcsm-lpd); programmed death 1 (pd-1); t-cell receptor gene rearrangement.
Copyright © 2025, Norimatsu et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Insitutional Review Board, International University of Health and Welfare, Japan issued approval 20-Nr-009. The authors obtained the necessary written in-force consent to report the case. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures









Similar articles
-
Expression of programmed death-1 in primary cutaneous CD4-positive small/medium-sized pleomorphic T-cell lymphoma, cutaneous pseudo-T-cell lymphoma, and other types of cutaneous T-cell lymphoma.Am J Surg Pathol. 2012 Jan;36(1):109-16. doi: 10.1097/PAS.0b013e318230df87. Am J Surg Pathol. 2012. PMID: 21989349
-
CD27/CD70 pathway activation in primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder.J Pathol. 2024 Feb;262(2):189-197. doi: 10.1002/path.6222. Epub 2023 Nov 7. J Pathol. 2024. PMID: 37933684
-
Cyclin D1 expression, cell proliferation, and clonal persistence characterize primary cutaneous CD4+ small or medium T-cell lymphoproliferative disorder.Histopathology. 2023 Feb;82(3):485-494. doi: 10.1111/his.14834. Epub 2022 Nov 18. Histopathology. 2023. PMID: 36341542
-
Primary Cutaneous CD4+ Small/Medium Pleomorphic T-Cell Lymphoproliferative Disorder: A Case Series.J Cutan Med Surg. 2017 Nov/Dec;21(6):502-506. doi: 10.1177/1203475417715209. Epub 2017 Jun 13. J Cutan Med Surg. 2017. PMID: 28605998 Review.
-
Cutaneous lymphoproliferative disorders: Back to the future.J Cutan Pathol. 2024 Jun;51(6):468-476. doi: 10.1111/cup.14609. Epub 2024 Mar 18. J Cutan Pathol. 2024. PMID: 38499969 Review.
References
-
- Primary cutaneous T-cell lymphomas other than mycosis fungoides and Sézary syndrome. Part I: clinical and histologic features and diagnosis. Stoll JR, Willner J, Oh Y, et al. J Am Acad Dermatol. 2021;85:1073–1090. - PubMed
-
- Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoma expresses follicular T-cell markers. Rodríguez Pinilla SM, Roncador G, Rodríguez-Peralto JL, et al. Am J Surg Pathol. 2009;33:81–90. - PubMed
-
- Epstein-Barr virus negative clonal plasma cell proliferations and lymphomas in peripheral T-cell lymphomas: a phenomenon with distinctive clinicopathologic features. Balagué O, Martínez A, Colomo L, et al. Am J Surg Pathol. 2007;31:1310–1322. - PubMed
-
- Expression of programmed death-1 in primary cutaneous CD4-positive small/medium-sized pleomorphic T-cell lymphoma, cutaneous pseudo-T-cell lymphoma, and other types of cutaneous T-cell lymphoma. Cetinözman F, Jansen PM, Willemze R. Am J Surg Pathol. 2012;36:109–116. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous