

Advancing multidisciplinary management of pediatric hyperinflammatory disorders
- PMID: 40370972
- PMCID: PMC12075326
- DOI: 10.3389/fped.2025.1553861
Advancing multidisciplinary management of pediatric hyperinflammatory disorders
Abstract
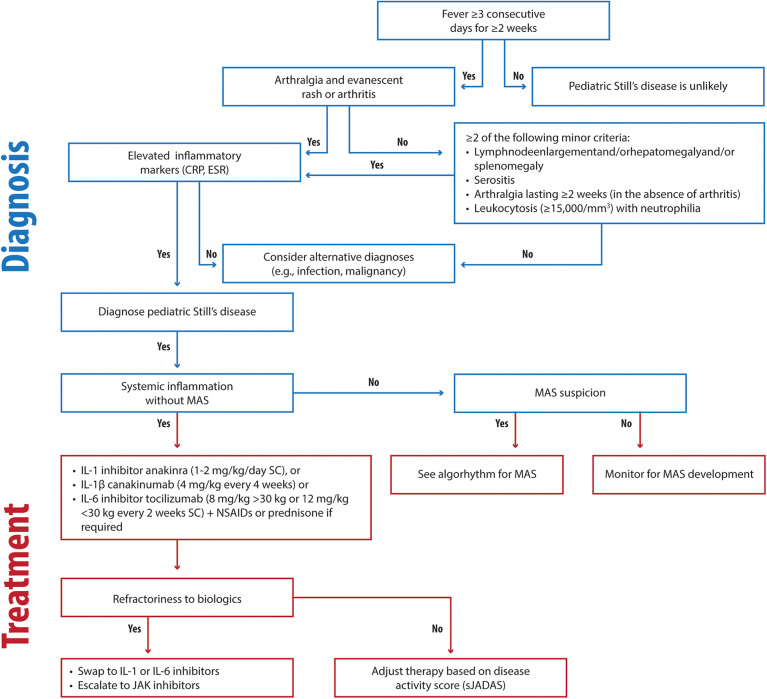
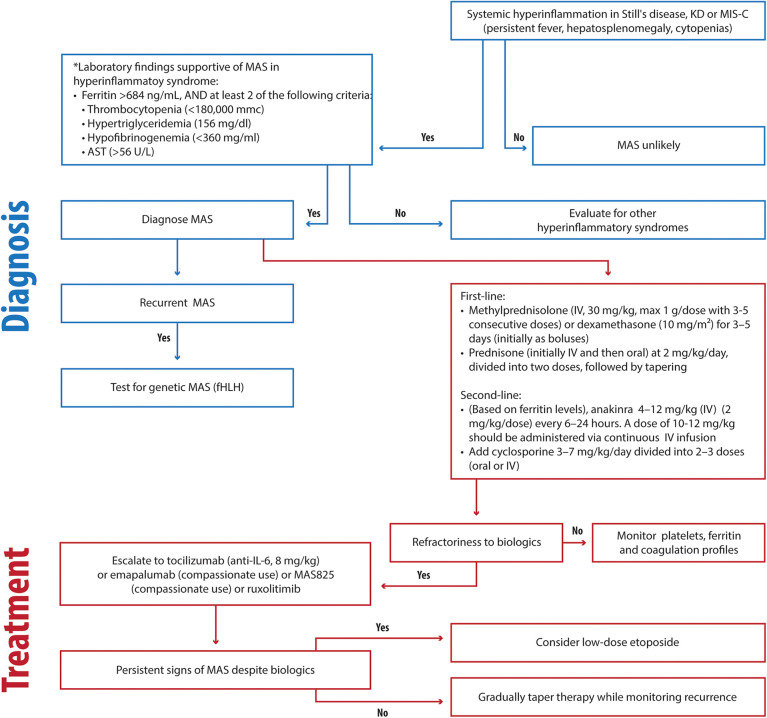
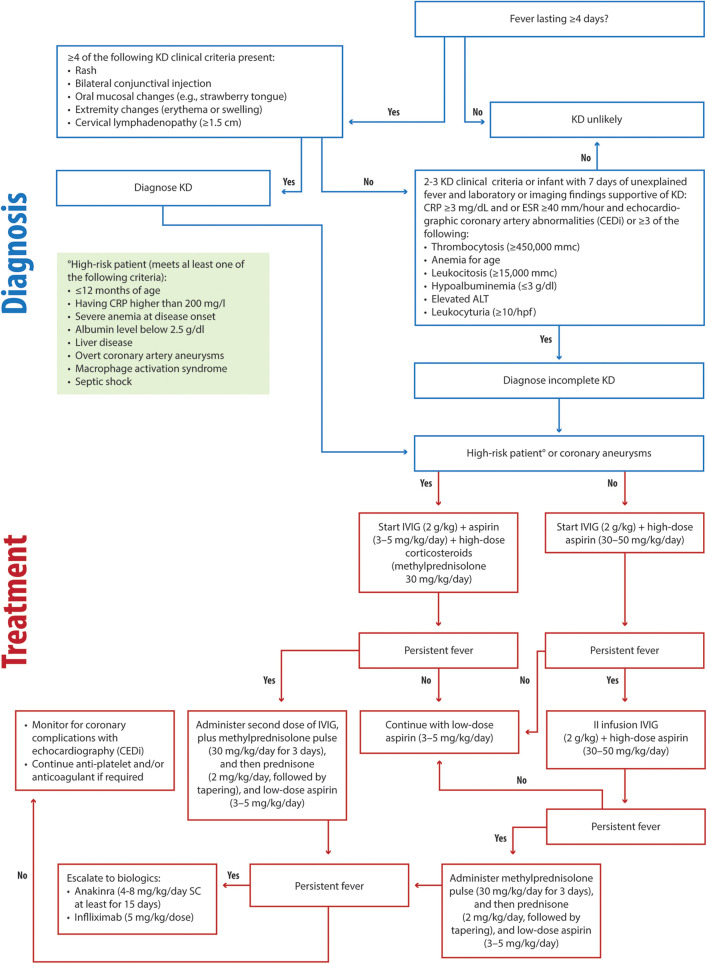
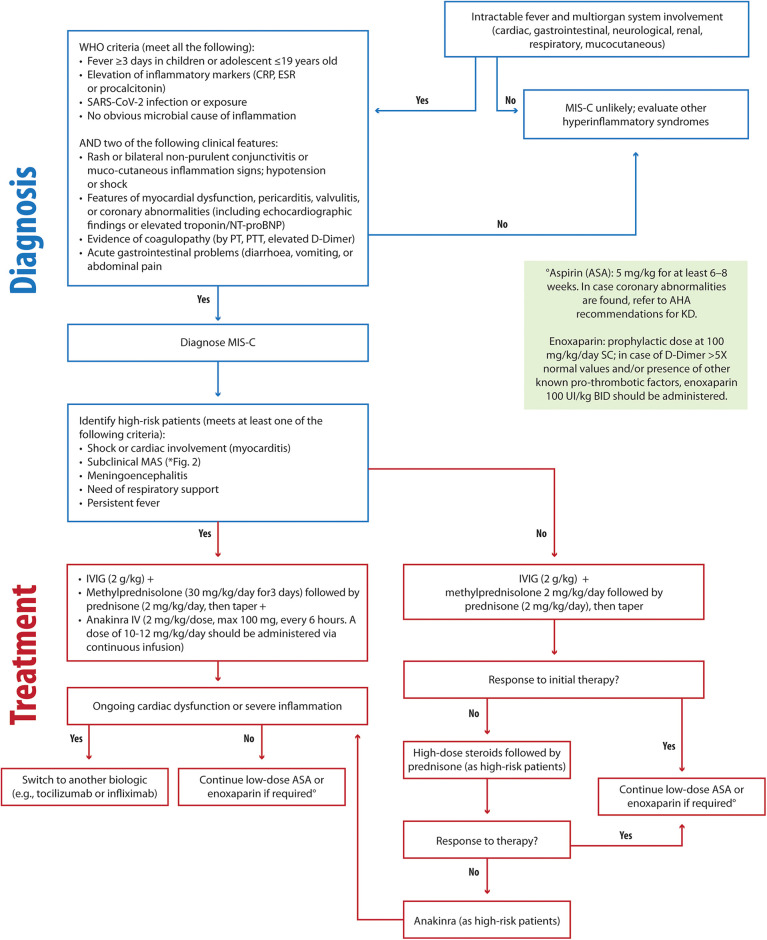
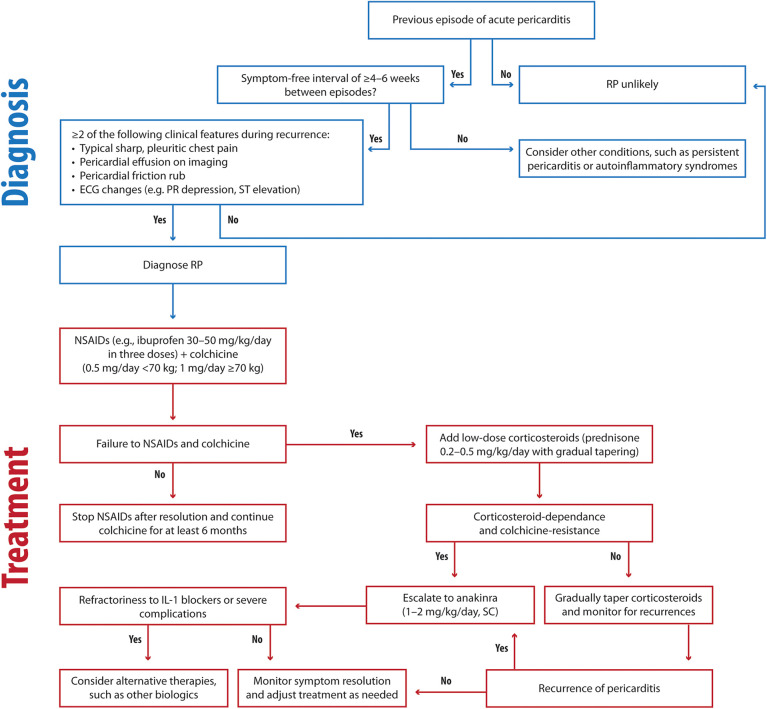
Pediatric hyperinflammatory diseases, including Still's disease, Kawasaki disease (KD), multisystem inflammatory syndrome in children (MIS-C), and recurrent pericarditis (RP), represent a spectrum of conditions characterized by immune dysregulation and systemic inflammation. Each disorder exhibits distinct pathophysiological mechanisms and clinical features, yet their overlapping presentations often pose diagnostic challenges. Early and accurate differentiation is critical to mitigate complications such as macrophage activation syndrome (MAS), coronary artery aneurysms, and myocardial dysfunction. This narrative review explores the pathophysiology, diagnostic criteria, and management of these conditions, emphasizing the utility of advanced biomarkers, imaging modalities, and genetic testing. For Still's disease, the review highlights the transformative role of biologic therapies targeting IL-1 and IL-6 in reducing systemic inflammation and improving outcomes. In KD, timely administration of intravenous immunoglobulin (IVIG) and combination with high-dose steroids in high-risk patients is pivotal for preventing coronary complications. MIS-C, associated with SARS-CoV-2 infection, requires tailored immunomodulatory approaches, including corticosteroids and biologics, to address severe hyperinflammation and multiorgan involvement. RP management prioritizes NSAIDs, colchicine, and IL-1 inhibitors to reduce recurrence and corticosteroid dependence. The review advocates for a multidisciplinary approach, integrating standardized diagnostic algorithms and disease-specific expertise to optimize patient care. Future research directions include the identification of predictive biomarkers, exploration of novel therapeutic targets, and development of evidence-based treatment protocols to enhance long-term outcomes in pediatric inflammatory diseases.
Keywords: IL-1; IL-6; Kawasaki disease; MIS-C multisystem inflammatory syndrome; biologics; hyperinflammation; recurrent pericarditis; still disease.
© 2025 La Torre, Meliota, Civino, Campanozzi, Cecinati, Rosati, Sacco, Santoro, Vairo and Cardinale.
Conflict of interest statement
FL has received speakers' fees from Sobi and Novartis. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Zhan W, Yang J, Qiu L, Yang K, Ye X, Shangguan Y, et al. Clinical characteristics and prognosis of interstitial lung disease in systemic juvenile idiopathic arthritis: a two-center retrospective observational cohort study. Pediatr Rheumatol Online J. (2024) 22:96. 10.1186/s12969-024-01028-5 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous