

Sensory driven neurophysiological mechanisms of concussion: a parsimonious and falsifiable theory
- PMID: 40371083
- PMCID: PMC12074929
- DOI: 10.3389/fneur.2025.1547786
Sensory driven neurophysiological mechanisms of concussion: a parsimonious and falsifiable theory
Abstract
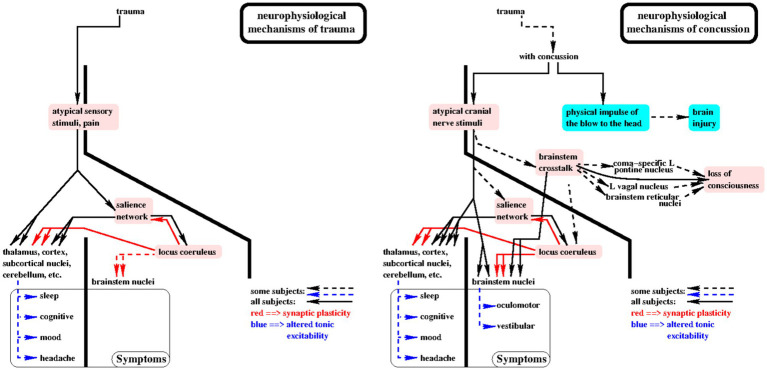
Every time a person sustains a blow to the head, they receive multiple atypical sensory inputs, often including pain. These directly stimulate the central nervous system. Yet, sensory input as a causal agent of neurophysiological dysfunction and post-concussion symptoms has never been explored. A new theory is proposed of sensory driven neurophysiological mechanisms of concussion (i) which are causally linked to the momentary blow to the head, (ii) whose time courses and other properties correspond to those observed to date for acute, sub-acute, and chronic symptoms, and (iii) which give rise to testable questions with experimentally measurable consequences. The primary assertion of the theory is that trauma induced excitation of key brain regions including the salience network (SN) and locus coeruleus (LC) can produce persistent dysfunctional alterations in the stable patterns of network excitability on which symptom-free neurological function depends. This mechanism is in play with any physical trauma, with or without a blow to the head. That is because atypical, painful, and otherwise high intensity sensory stimuli excite the SN and thence the LC, inducing plasticity widely in the brain. Many of those sensory stimuli may persist through the recovery period and while the brain is plastic, enable one or another network to learn altered and potentially dysfunctional patterns of network excitability. The secondary assertion of the theory is that with a blow to the head, convergence of high-intensity sensory stimuli within the brainstem and midbrain can cause neurophysiological coupling between brainstem nuclei which normally function independently, i.e. brainstem crosstalk (BCT). It is BCT which causes the signs and symptoms specific to head trauma, e.g., loss of consciousness, and oculomotor and vestibular dysfunction. The theory's reliance on sensory input emphasizes the importance of putative mechanisms whose initiating cause is known to have been present for every head trauma. This is in contrast to the century-long focus on mechanisms whose initiating cause, brain injury, is undetectable by clinical exam, neuroimaging, and bioassay in fully 60% of all head trauma, i.e., 70-75% of all mild TBI. As formulated and described, the theory is readily testable and falsifiable.
Keywords: CamCAN; concussion; head trauma; magnetoencephalagraphy; neurophysiology; traumatic brain injury.
Copyright © 2025 Krieger, Shepard, Kontos, Collins, Puccio, Eagle, Schneider and Okonkwo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, et al. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. (2016) 51:838–847. - PubMed
-
- Matney C, Bowman K, Berwick D. In: Bowman K, Berwick D, Matney C, editors. National Academies of sciences, engineering, and medicine; health and medicine division; board on health care services; board on health sciences policy; committee on accelerating Progress in traumatic brain injury research and care. Washington, DC: National Academies Press (US) (2022)
LinkOut - more resources
Full Text Sources
Research Materials