

Virome drift in ulcerative colitis patients: faecal microbiota transplantation results in minimal phage engraftment dominated by microviruses
- PMID: 40371968
- PMCID: PMC12087655
- DOI: 10.1080/19490976.2025.2499575
Virome drift in ulcerative colitis patients: faecal microbiota transplantation results in minimal phage engraftment dominated by microviruses
Abstract
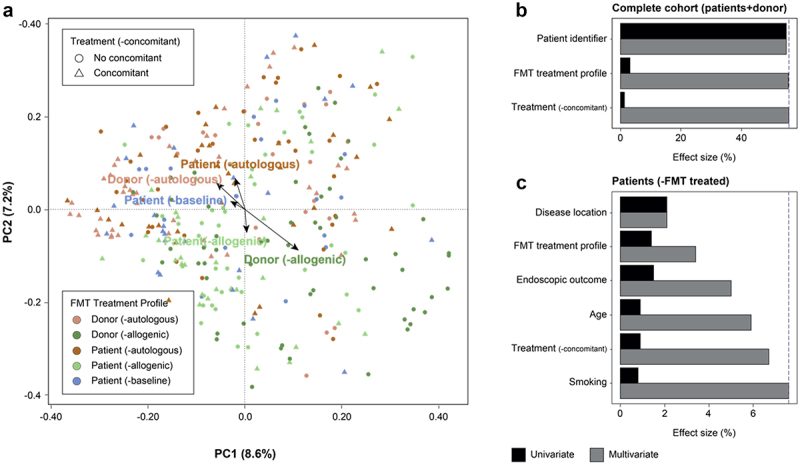
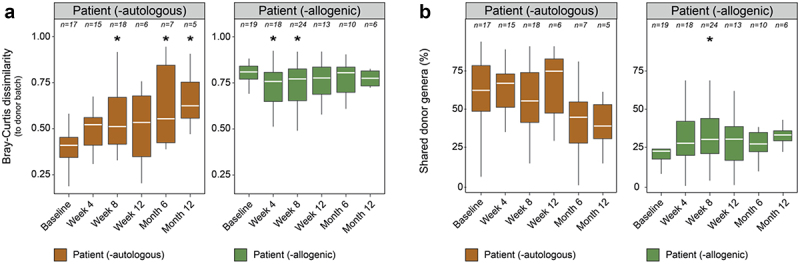
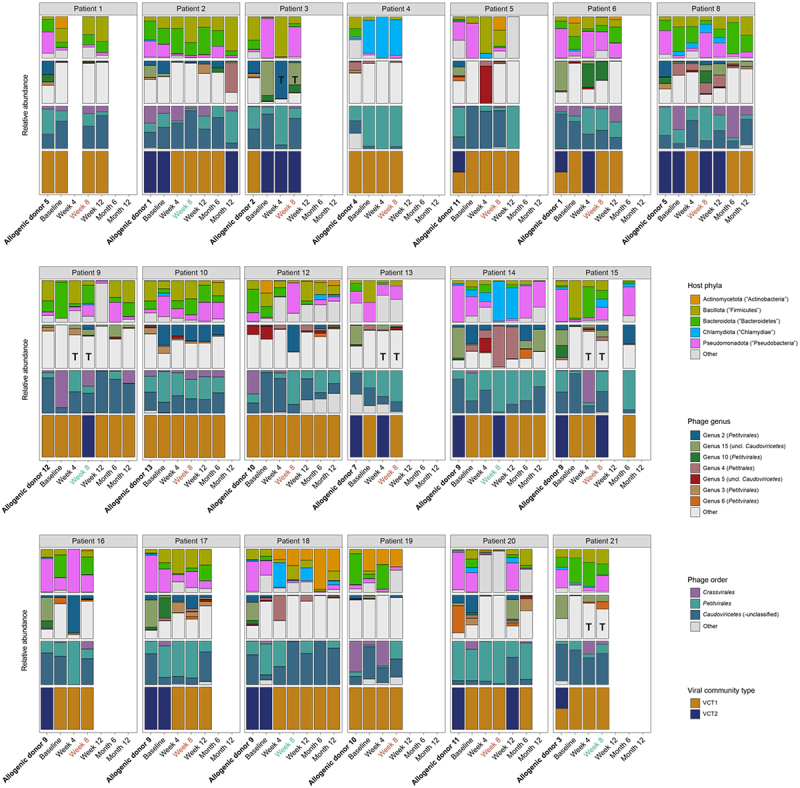
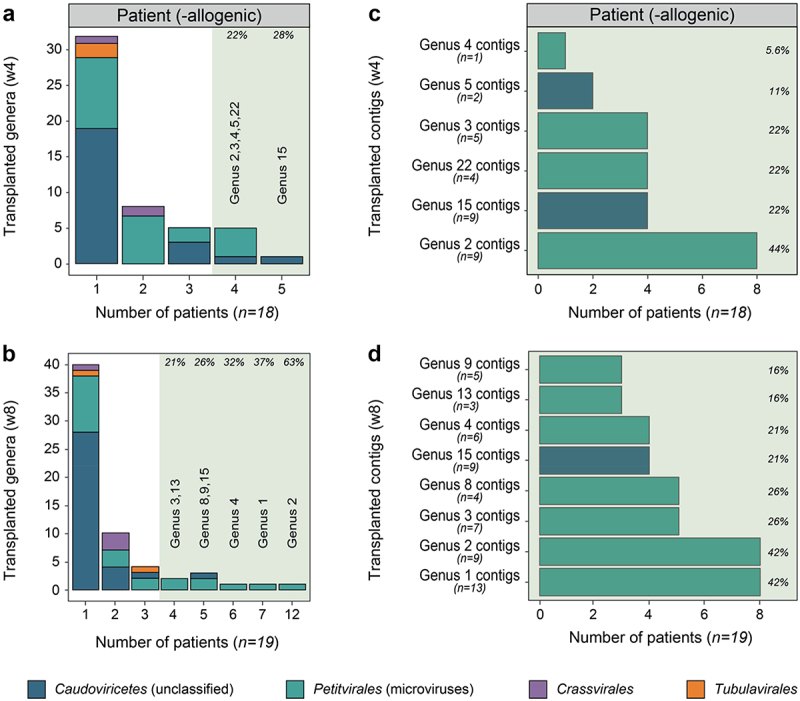
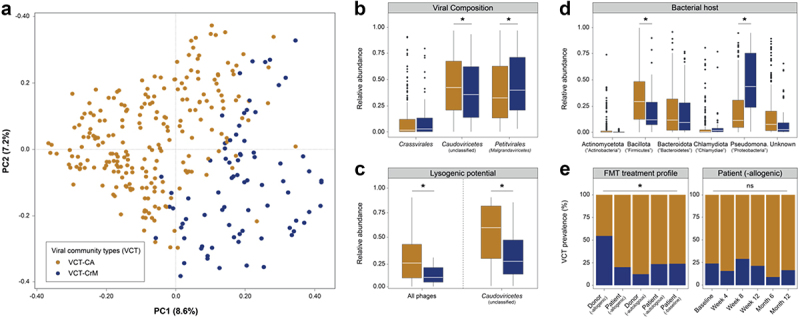
Ulcerative colitis (UC) is an inflammatory bowel disease characterized by recurrent colonic inflammation. Standard treatments focus on controlling inflammation but remain ineffective for one-third of patients. This underscores the need for alternative approaches, such as fecal microbiota transplantation (FMT), which transfers healthy donor microbiota to patients. The role of viruses in this process, however, remains underexplored. To address this, we analyzed the gut virome using metagenomic sequencing of enriched viral particles from 320 longitudinal fecal samples of 44 patients enrolled in the RESTORE-UC FMT trial. Patients were treated with FMTs from healthy donors (allogenic, treatment) or themselves (autologous, control). We found that colonic inflammation, both its presence and location, had a greater impact on the gut virome than FMT itself. In autologous FMT patients, the virome was unstable and showed rapid divergence over time, a phenomenon we termed virome drift. In allogenic FMT patients, the virome temporarily shifted toward the healthy donor, lasting up to 5 weeks and primarily driven by microviruses. Notably, two distinct virome configurations were identified and linked to either healthy donors or patients. In conclusion, inflammation strongly affects the gut virome in UC patients, which may lead to instability and obstruct the engraftment of allogeneic FMT.
Keywords: Ulcerative colitis; fecal microbiota transplants; virome; virome community types; virome drift.
Conflict of interest statement
Sara Deleu has been listed as a co-inventor on an international patent application entitled ‘Improved probiotic potency of yeast
Figures
References
-
- Alatab S, Sepanlou SG, Ikuta K, Vahedi H, Bisignano C, Safiri S, Sadeghi A, Nixon MR, Abdoli A, Abolhassani H, et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–19. doi: 10.1016/S2468-1253(19)30333-4. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical