

Clinical efficacy and learning curve analysis of 101 robotic-assisted Warshaw procedures: a retrospective study
- PMID: 40372447
- PMCID: PMC12222389
- DOI: 10.1007/s00464-025-11790-6
Clinical efficacy and learning curve analysis of 101 robotic-assisted Warshaw procedures: a retrospective study
Abstract
Objective: To evaluate the clinical efficacy of robotic-assisted Warshaw procedure and analyze its learning curve.
Methods: This retrospective case series analyzed 101 consecutive patients who underwent robotic-assisted Warshaw procedure at the Department of Hepatobiliary and Pancreatic Surgery, Affiliated Hospital of Qingdao University, between November 2020 and January 2023. Patient demographics, perioperative outcomes, pathological findings, and follow-up data were collected. For continuous variables such as operative time and blood loss, the cumulative sum (CUSUM) method and best-fit curve analysis were employed to assess the learning curve. For categorical variables including major complications and textbook outcome, a 2-piece linear model was used. Patients were stratified into early learning phase and proficiency phase groups based on the identified inflection points, and perioperative outcomes were compared between groups.
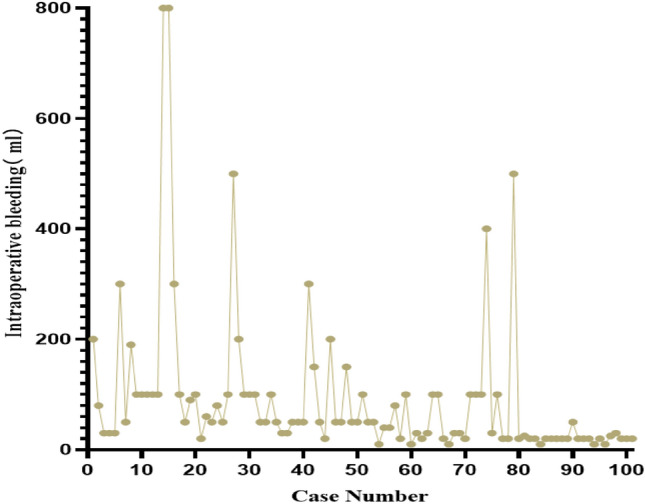
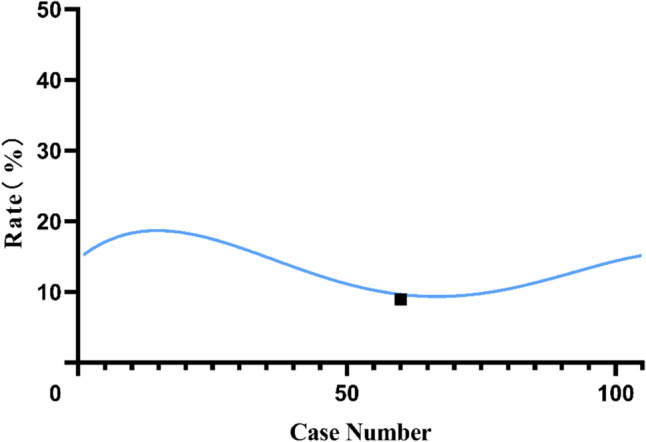
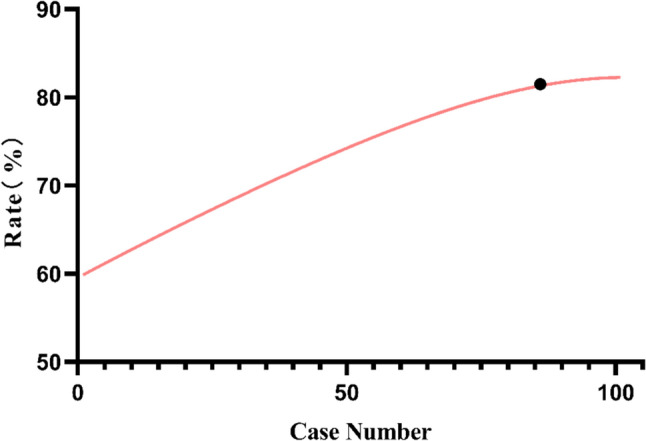
Results: (1) Patient demographics and perioperative outcomes: Among 101 patients (21 males [20.79%] and 80 females [79.21%], mean age 48.90 ± 11.97 years), the mean operative time was 187.09 ± 52.36 min and median blood loss was 50 ml (IQR: 20-100 ml). The Warshaw procedure was successfully completed in 91 patients (90.10%), while 7 patients (6.93%) required conversion to distal pancreatectomy with splenectomy, and 3 patients (2.97%) were converted to open surgery. Postoperative pancreatic fistula (POPF) occurred in 18 patients (17.82%), including 13 biochemical leaks (12.87%) and 5 grade B fistulas (4.95%), with no grade C fistulas. No chylous fistula or delayed gastric emptying was observed. Postoperative hemorrhage occurred in 5 patients (4.95%) and intra-abdominal infection in 3 patients (2.97%), with 2 patients (1.98%) experiencing both complications requiring reoperation. One patient (0.99%) developed bowel obstruction. The mean time to first oral intake was 2.35 ± 0.69 days. Fifty-six patients (55.44%) were discharged with drains. Median postoperative hospital stay was 6.00 days (IQR: 5.00-7.50), and mean drainage duration was 9.88 ± 2.92 days. All patients were discharged without perioperative mortality or 90 day readmission. During follow-up, 10 patients (16.13%, 10/62) developed varying degrees of splenic infarction, and 13 patients (20.96%, 13/62) developed gastric varices, but no severe complications such as splenic abscess or gastrointestinal bleeding occurred. (2) Learning curve analysis: For operative time and blood loss, CUSUM learning curves were best fitted by the equations: CUSUM(operative time) = 0.003156X3 - 1.141X2 + 83.71X - 1.092 and CUSUM(blood loss) = 0.01250X3 - 2.889X2 + 167.4X - 33.65 (where X represents case number), with R2 values of 0.936 and 0.927, respectively (P < 0.05). The CUSUM value for operative time peaked at case 45, while that for blood loss peaked at case 39. For postoperative complications, the learning curve inflection point was case 60, while for textbook outcome, it was case 85. (3) Comparison between learning phases: Using operative time (case 45) as the cutoff point, there were no significant differences in ASA scores or POPF rates between the two phases (P > 0.05). However, significant improvements were observed in operative time, blood loss, and drainage duration in the proficiency phase (P < 0.05). Using textbook outcome (case 85) as the cutoff point, significant improvements were seen in operative time, blood loss, and textbook outcome achievement (P < 0.05).
Conclusion: (1) The robotic-assisted Warshaw procedure is safe and feasible. (2) Learning curve analysis revealed that proficiency in operative time and blood loss was achieved earlier, followed by postoperative complications (60 cases), while mastery of textbook outcomes required the most experience (85 cases).
Keywords: Clinical efficacy; Learning curve; Robotic surgery; Safety; Warshaw procedure.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Disclosures: Drs. Hongliang Liu, Qisheng Hao, Xi Wang, Mengxing Cheng, Fabo Qiu and Bin Zhou have no conflicts of interest or financial ties to disclose.
Figures



Similar articles
-
Learning curve of robotic assisted total knee arthroplasty within a surgical team: A prospective study of 115 cases.Orthop Traumatol Surg Res. 2025 Sep;111(5):104325. doi: 10.1016/j.otsr.2025.104325. Epub 2025 Jun 30. Orthop Traumatol Surg Res. 2025. PMID: 40602664
-
Learning Curve of Single-Port Robotic-Assisted Extraperitoneal Radical Prostatectomy: A CUSUM-Based Analysis.J Laparoendosc Adv Surg Tech A. 2025 Jul;35(7):542-549. doi: 10.1089/lap.2025.0055. Epub 2025 May 15. J Laparoendosc Adv Surg Tech A. 2025. PMID: 40372956
-
Limited versus full sternotomy for aortic valve replacement.Cochrane Database Syst Rev. 2017 Apr 10;4(4):CD011793. doi: 10.1002/14651858.CD011793.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2023 Dec 6;12:CD011793. doi: 10.1002/14651858.CD011793.pub3. PMID: 28394022 Free PMC article. Updated.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Initial 50 consecutive full-robotic pancreatoduodenectomies without conversion by a single surgeon: a learning curve analysis from a tertiary referral high-volume center.Surg Endosc. 2023 May;37(5):3531-3539. doi: 10.1007/s00464-022-09784-9. Epub 2023 Jan 3. Surg Endosc. 2023. PMID: 36596929 Free PMC article.
References
-
- Zhao Y (2008) Paying attention to the diagnosis and treatment of benign pancreatic tumors. China J Pract Surg 05:333–335
-
- Tang Y, Zhang Z, Wu X et al (2018) The evaluation of the short-term operative complications and the long-term quality of life of the organ-preserving pancreatectomy. Chin J Pancreatol 2018:318–323
-
- Yoh T, Cauchy F, Soubrane O (2022) Oncological resection for liver malignancies: can the laparoscopic approach provide benefits? Ann Surg 275(1):182–188 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
