

Effects of an interprofessional care concept in nursing homes evaluated in the SaarPHIR project: A cluster-randomized controlled trial
- PMID: 40373071
- PMCID: PMC12080800
- DOI: 10.1371/journal.pone.0321118
Effects of an interprofessional care concept in nursing homes evaluated in the SaarPHIR project: A cluster-randomized controlled trial
Abstract
Introduction: Deficits in interprofessional collaboration can lead to insufficient medical care for nursing home residents, particularly inappropriate hospitalizations. Transfers are stressful for residents, and hospital stays can lead to infections and functional decline. Increasing the role of general practitioners and improving collaboration between professionals may reduce hospitalizations. In an effort to reduce hospitalizations and improve quality of care for nursing home residents, the SaarPHIR project implemented and evaluated a complex intervention which aimed at improving cooperation between general practitioners and nurses. This paper evaluates the effectiveness of an interprofessional care concept in nursing homes.
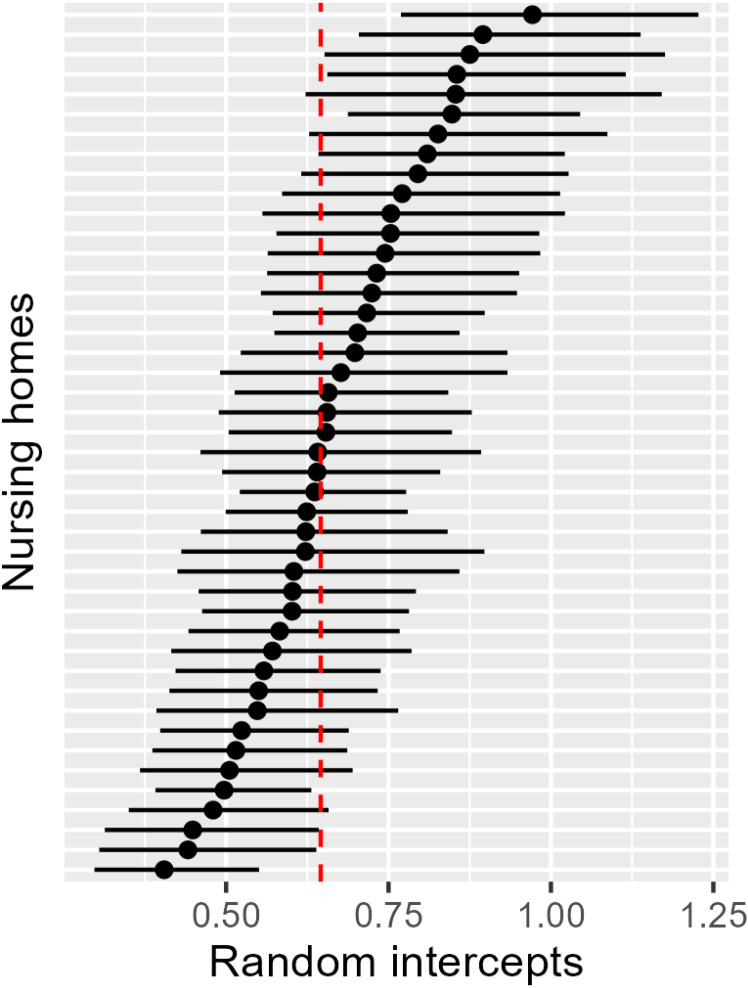
Methods: A prospective, cluster-randomized controlled trial was conducted in Saarland, Germany, from May 2019 until July 2020 with a 15-months of follow-up, with two parallel groups and a 1:1 randomization at district level to evaluate the effectiveness of the intervention. The six administrative districts of the German federal state of Saarland were selected as randomization clusters to avoid spillover effects. The primary outcome, hospitalization, was assessed using claims data from six health insurers. Analyses were performed using generalized linear mixed models assuming both a Poisson and, for sensitivity analyses, a negative binomial distribution allowing for clustering at the nursing home level. Considering the randomized cluster level in the primary analysis would be the proper approach. However, after careful consideration, an unconventional approach was adopted to ensure the evaluation of the intervention within the complex healthcare system with a pragmatic design. The randomized cluster level was considered in sensitivity analyses. Secondary outcomes included ambulatory care-sensitive and nursing home care-sensitive admissions, mortality and hospital days. Furthermore, health economic aspects were explored by comparing costs between groups descriptively and exploratively using a generalized linear mixed model with a log-link and a gamma distribution.
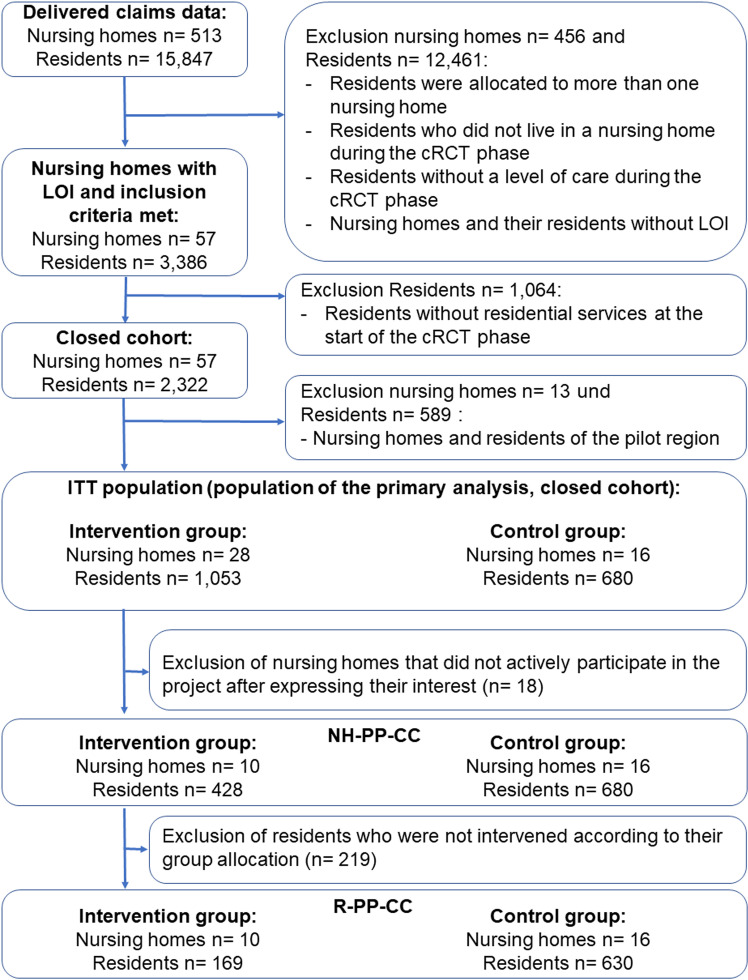
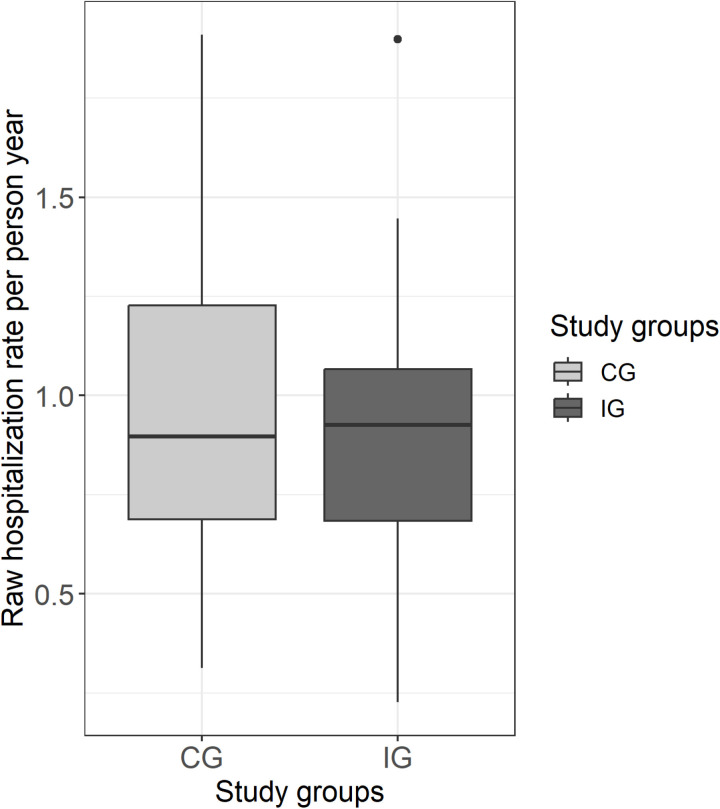
Results: Twenty-eight nursing homes received the intervention (1,053 residents), and 16 nursing homes (680 residents) were assigned to usual care. Hospitalization rates did not differ significantly between groups (incidence rate ratio [IRR] = 0.94; 95% CI: 0.78-1.14). Nursing home care-sensitive admissions could be reduced in residents treated with the interprofessional care concept (IRR: 0.73, 95% CI: 0.59-0.96). No differences in mortality, number of days spent in hospital and healthcare costs were found between groups. Mean drug costs (€82.53; 95% CI: 11.79-165.06) were higher and costs for ambulatory hospital stays lower (-€40.80; 95% CI: -76.50-0.00) in the intervention group.
Conclusion: All-cause hospitalization was not significantly affected in the relatively short duration of the intervention. Nevertheless, secondary outcomes suggest some positive effects for the intervention group. However, participation in the intervention group was lower than expected at both the nursing home and resident levels, limiting the validity of the results.
Copyright: © 2025 Tönnies et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Effect of an interprofessional care concept on the hospitalization of nursing home residents: study protocol for a cluster-randomized controlled trial.Trials. 2020 May 18;21(1):411. doi: 10.1186/s13063-020-04325-y. Trials. 2020. PMID: 32423463 Free PMC article.
-
Effects of strategies to improve general practitioner-nurse collaboration and communication in regard to hospital admissions of nursing home residents (interprof ACT): study protocol for a cluster randomised controlled trial.Trials. 2020 Nov 5;21(1):913. doi: 10.1186/s13063-020-04736-x. Trials. 2020. PMID: 33153484 Free PMC article.
-
Effect of a clinical pathway to reduce hospitalizations in nursing home residents with pneumonia: a randomized controlled trial.JAMA. 2006 Jun 7;295(21):2503-10. doi: 10.1001/jama.295.21.2503. JAMA. 2006. PMID: 16757722 Clinical Trial.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
A complex intervention to reduce avoidable hospital admissions in nursing homes: a research programme including the BHiRCH-NH pilot cluster RCT.Southampton (UK): NIHR Journals Library; 2021 Feb. Southampton (UK): NIHR Journals Library; 2021 Feb. PMID: 33651525 Free Books & Documents. Review.
References
-
- Jacobs K, Kuhlmey A, Greß S, Klauber J, Schwinger A. Pflege-Report 2021: Sicherstellung der Pflege: Bedarfslagen und Angebotsstrukturen. 2021;2021.
-
- Klauber J, Wasem J, Beivers A, Mostert C, . Krankenhaus-Report 2021: Versorgungsketten – Der Patient im Mittelpunkt. 2021.
-
- Ouslander JG, Lamb G, Perloe M, Givens JH, Kluge L, Rutland T, et al.. Potentially avoidable hospitalizations of nursing home residents: frequency, causes, and costs: see editorial comments by Drs. Jean F. Wyman and William R. Hazzard, pp 760-761. J Am Geriatr Soc. 2010;58(4):627–35. doi: 10.1111/j.1532-5415.2010.02768.x - DOI - PubMed
-
- Gombault-Datzenko E, Costa N, Mounié M, Tavassoli N, Mathieu C, Roussel H, et al.. Cost of care pathways before and after appropriate and inappropriate transfers to the emergency department among nursing home residents: results from the FINE study. BMC Geriatr. 2024;24(1):353. doi: 10.1186/s12877-024-04946-x - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
