

Endometrial Metabolism of 17β-Estradiol during the Window of Implantation in Women with Recurrent Implantation Failure
- PMID: 40373756
- PMCID: PMC12215175
- DOI: 10.1159/000546442
Endometrial Metabolism of 17β-Estradiol during the Window of Implantation in Women with Recurrent Implantation Failure
Abstract
Objectives: Alterations in 17β-estradiol metabolism are known to potentially impair endometrial receptivity. Previous pioneering studies have investigated the role of endometrial steroid metabolism by determining steroid hormone levels and steroid-metabolizing enzyme activity in endometrial biopsies of patients undergoing IVF. The activity of oxidative and reductive 17β-hydroxysteroid dehydrogenases (17β-HSDs), which catalyze the interconversion between estrone and 17β-estradiol, was found to be similar between IVF patients who - after fresh embryo transfer in the cycle following endometrial biopsy - did and did not become pregnant. However, inhibition of the reductive enzyme 17β-hydroxysteroid dehydrogenase type 1 (17β-HSD1), the most prominent 17β-HSD type in 17β-estradiol formation, was found to differ between groups. The primary objective of this study was to determine oxidative and reductive 17β-HSD enzyme activity in the endometrium of two well-defined groups: IVF patients with recurrent implantation failure (RIF) and control patients.
Design: This is a prospective observational study of IVF patients with RIF (n = 52) and controls (n = 25). Patients undergoing treatment because of pre-implantation genetic testing, a severe male factor, or bilateral tubal pathology were recruited as controls since these conditions did not suggest an endometrial contribution to infertility.
Participants/materials, setting, methods: Endometrial biopsies were obtained 5-8 days after a positive urine ovulation test in a natural cycle using a Pipelle catheter. Activity of oxidative and reductive enzymes, inhibition of 17β-HSD1, 5, 7, and 12, and immunostaining of 17β-HSD7 were performed. The formation of 17β-estradiol by reduction of estrone (reductive enzymes), formation of estrone by oxidation of 17β-estradiol (oxidative enzymes), and inhibition of specific 17β-HSD enzymes were determined using high-performance liquid chromatography. Formalin-fixed paraffin-embedded tissue was used for immunostaining. The Student's t test and Mann-Whitney U test were used for statistical analysis. Multivariate analysis was used to determine the influence of confounders.
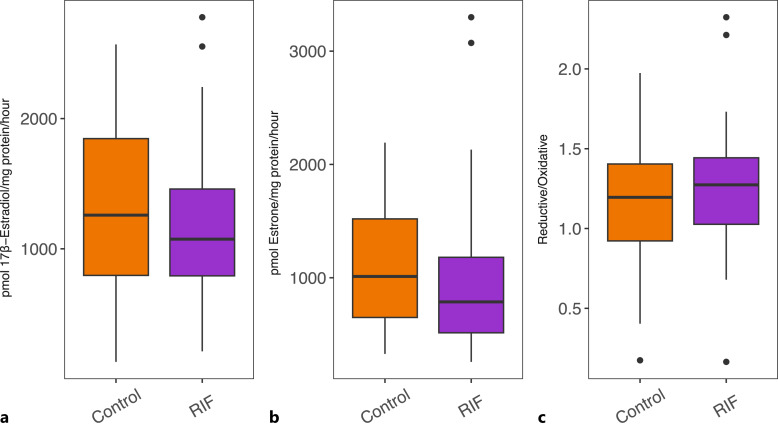
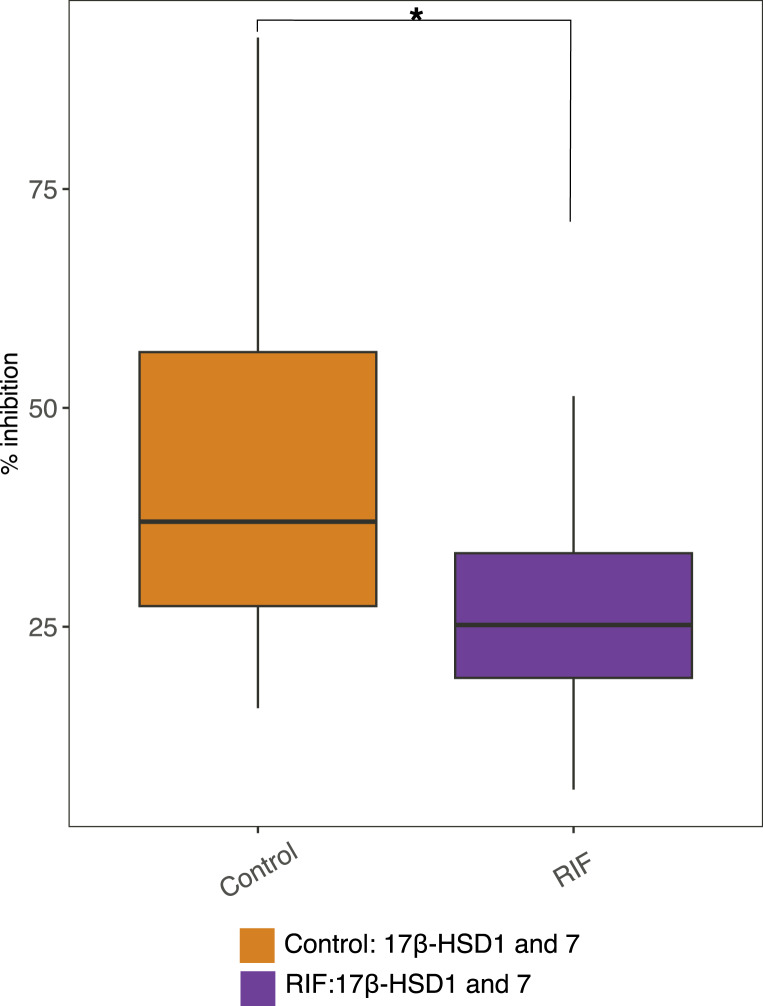
Results: No differences were found in activity of oxidative and reductive 17β-HSD enzymes in RIF patients and controls. Combined inhibition of 17β-HSD5, 7, and 12 was significantly lower in the RIF group compared to controls (p = 0.04). Inhibition of 17β-HSD1 and 17β-HSD7 combined was also significantly lower (more production of 17β-estradiol remained) in the RIF group compared to controls (p < 0.01). However, solely inhibiting 17β-HSD1 or 17β-HSD7 showed no significant difference between groups. Immunostaining revealed the expression of 17β-HSD7 in all endometrial samples.
Limitations: Results should be interpreted carefully due to possible cycle-to-cycle variation, challenges to translate in vitro findings to biological conditions, and the heterogeneous etiology of RIF.
Conclusions: Differences in formation of 17β-estradiol in the presence of two specific inhibitors of 17β-HSD1 and 7 between RIF patients and controls were found. Although 17β-HSD1, expressed at the fetal-maternal interface, has been associated with fertility, the potential role of 17β-HSD7 in human implantation has not been previously described. The observed differences between patients with RIF and controls warrant future research on the role of this main enzyme and its lesser-known 17β-HSD type in endometrial receptivity and implantation.
Keywords: 17β-Estradiol; Endometrium; Implantation; In vitro fertilization; Intracrinology.
© 2025 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures



Similar articles
-
Podocalyxin is a key negative regulator of human endometrial epithelial receptivity for embryo implantation.Hum Reprod. 2021 Apr 20;36(5):1353-1366. doi: 10.1093/humrep/deab032. Hum Reprod. 2021. PMID: 33822049 Free PMC article.
-
Cycle regimens for frozen-thawed embryo transfer.Cochrane Database Syst Rev. 2017 Jul 5;7(7):CD003414. doi: 10.1002/14651858.CD003414.pub3. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2025 Jun 3;6:CD003414. doi: 10.1002/14651858.CD003414.pub4. PMID: 28675921 Free PMC article. Updated.
-
Endometrial injury for pregnancy following sexual intercourse or intrauterine insemination.Cochrane Database Syst Rev. 2016 Jun 14;(6):CD011424. doi: 10.1002/14651858.CD011424.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2021 Mar 18;3:CD011424. doi: 10.1002/14651858.CD011424.pub3. PMID: 27296541 Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Endometrial injury for pregnancy following sexual intercourse or intrauterine insemination.Cochrane Database Syst Rev. 2022 Oct 24;10(10):CD011424. doi: 10.1002/14651858.CD011424.pub4. Cochrane Database Syst Rev. 2022. PMID: 36278845 Free PMC article.
Cited by
-
Precision Therapeutic and Preventive Molecular Strategies for Endometriosis-Associated Infertility.Int J Mol Sci. 2025 Aug 9;26(16):7706. doi: 10.3390/ijms26167706. Int J Mol Sci. 2025. PMID: 40869026 Free PMC article. Review.
References
-
- Delhanty JD, Harper JC, Ao A, Handyside AH, Winston RM. Multicolour FISH detects frequent chromosomal mosaicism and chaotic division in normal preimplantation embryos from fertile patients. Hum Genet. 1997;99(6):755–60. - PubMed
-
- Pirtea P, De Ziegler D, Tao X, Sun L, Zhan Y, Ayoubi JM, et al. Rate of true recurrent implantation failure is low: results of three successive frozen euploid single embryo transfers. Fertil Steril. 2021;115(1):45–53. - PubMed
-
- Cimadomo D, Rienzi L, Conforti A, Forman E, Canosa S, Innocenti F, et al. Opening the black box: why do euploid blastocysts fail to implant? A systematic review and meta-analysis. Hum Reprod Update. 2023;29(5):570–633. - PubMed
-
- Devroey P, Bourgain C, Macklon NS, Fauser BC. Reproductive biology and IVF: ovarian stimulation and endometrial receptivity. Trends Endocrinol Metab. 2004;15(2):84–90. - PubMed
LinkOut - more resources
Full Text Sources
